

Subtype Classification of Lung Adenocarcinoma Predicts Benefit From Adjuvant Chemotherapy in Patients Undergoing Complete Resection
- PMID: 25918286
- PMCID: PMC4606061
- DOI: 10.1200/JCO.2014.58.8335
Subtype Classification of Lung Adenocarcinoma Predicts Benefit From Adjuvant Chemotherapy in Patients Undergoing Complete Resection
Abstract
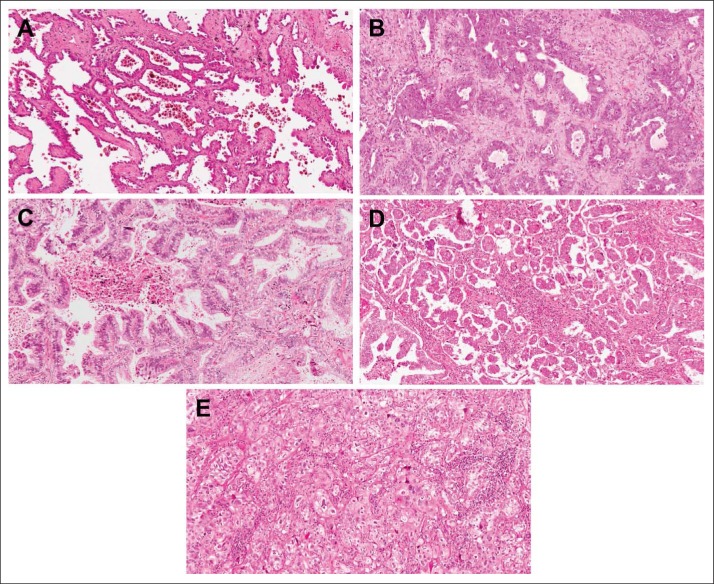
Purpose: The classification for invasive lung adenocarcinoma by the International Association for the Study of Lung Cancer, American Thoracic Society, European Respiratory Society, and WHO is based on the predominant histologic pattern-lepidic (LEP), papillary (PAP), acinar (ACN), micropapillary (MIP), or solid (SOL)-present in the tumor. This classification has not been tested in multi-institutional cohorts or clinical trials or tested for its predictive value regarding survival from adjuvant chemotherapy (ACT).
Patients and methods: Of 1,766 patients in the IALT, JBR.10, CALGB 9633 (Alliance), and ANITA ACT trials included in the LACE-Bio study, 725 had adenocarcinoma. Histologies were reclassified according to the new classification and then collapsed into three groups (LEP, ACN/PAP, and MIP/SOL). Primary end point was overall survival (OS); secondary end points were disease-free survival (DFS) and specific DFS (SDFS). Hazard ratios (HRs) and 95% CIs were estimated through multivariable Cox models stratified by trial. Prognostic value was estimated in the observation arm and predictive value by a treatment effect interaction with histologic subgroups. Significance level was set at .01 for pooled analysis.
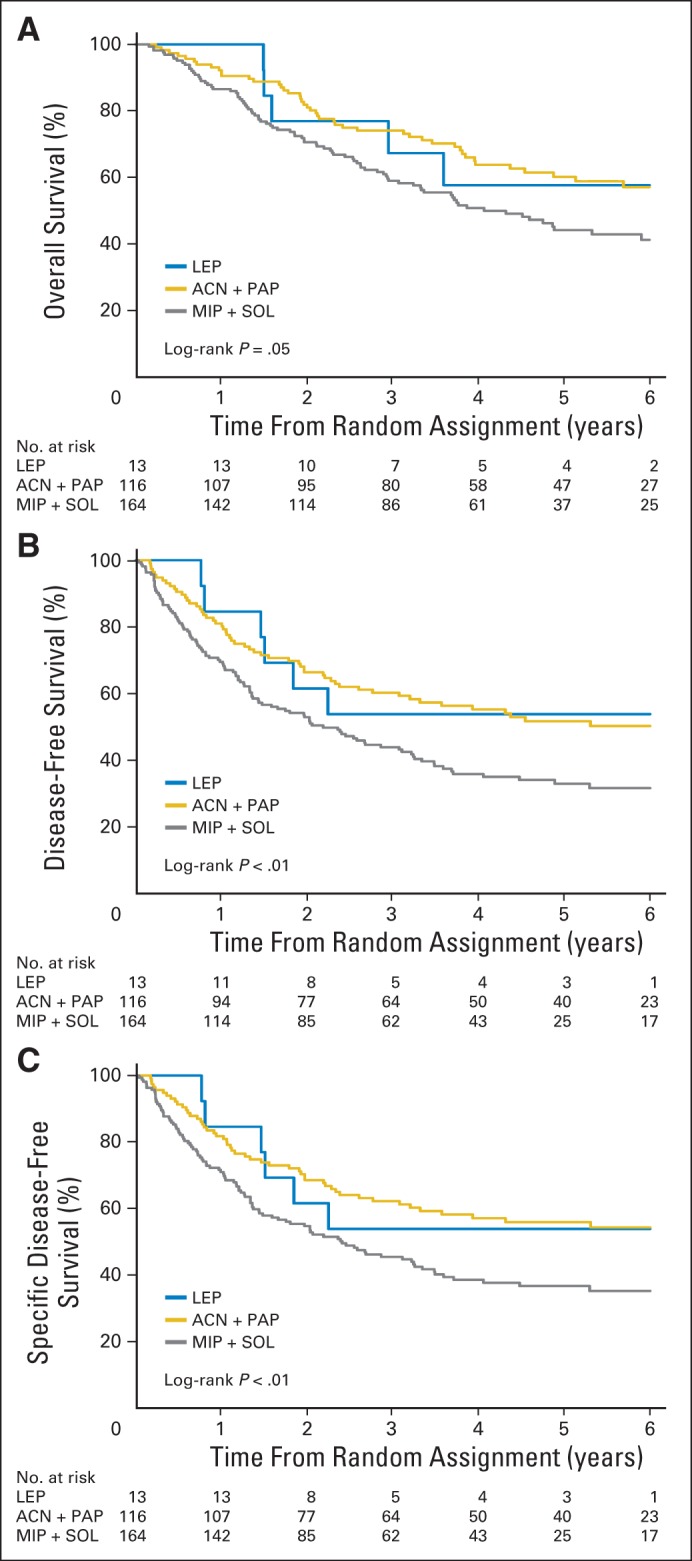
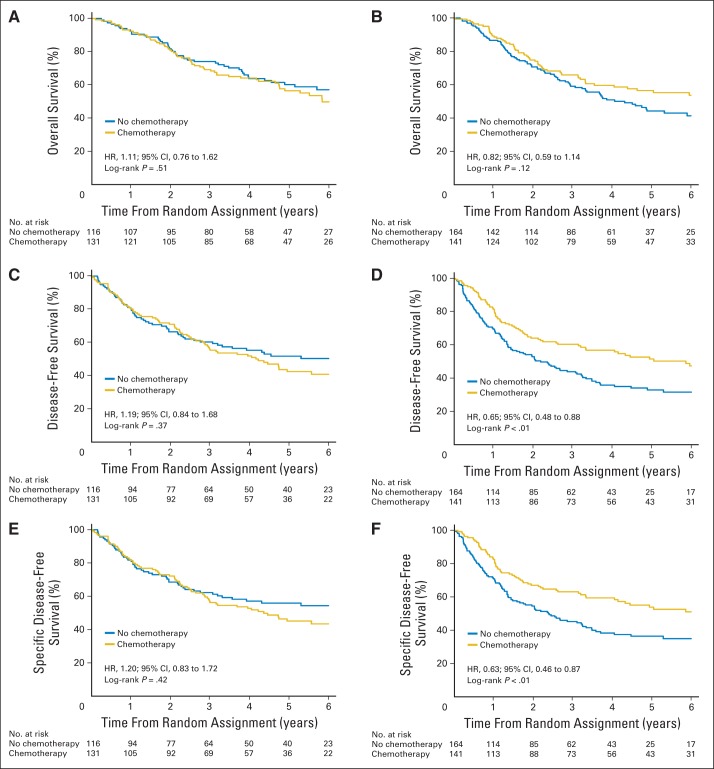
Results: A total of 575 patients were included in this analysis. OS was not prognostically different between histologic subgroups, but univariable DFS and SDFS were worse for MIP/SOL compared with LEP or ACN/PAP subgroup (P < .01); this remained marginally significant after adjustment. MIP/SOL patients (but not ACN/PAP) derived DFS and SDFS but not OS benefit from ACT (OS: HR, 0.71; 95% CI, 0.51 to 0.99; interaction P = .18; DFS: HR, 0.60; 95% CI, 0.44 to 0.82; interaction P = < .01; and SDFS: HR, 0.59; 95% CI, 0.42 to 0.81; interaction P = .01).
Conclusion: The new lung adenocarcinoma classification based on predominant histologic pattern was not predictive for ACT benefit for OS, but it seems predictive for disease-specific outcomes.
© 2015 by American Society of Clinical Oncology.
Conflict of interest statement
Authors' disclosures of potential conflicts of interest are found in the article online at
Figures
References
-
- Travis WD, Brambilla E, Muller-Hermelink HK, et al., editors. WHO Classification of Tumours 2004: Pathology and Genetics of Tumours of the Lung, Pleura, Thymus and Heart. Lyon, France: IARC Press; 2004.
-
- Travis WD, Brambilla E, Burke A, et al., editors. WHO Classification of the Tumours of the Lung, Pleura, Thymus and Heart (ed 4) Lyon, France: IARC Press; 2015. - PubMed
-
- Yoshizawa A, Motoi N, Riely GJ, et al. Impact of proposed IASLC/ATS/ERS classification of lung adenocarcinoma: Prognostic subgroups and implications for further revision of staging based on analysis of 514 stage I cases. Mod Pathol. 2011;24:653–664. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
