

Transcranial magnetic stimulation of the brain: guidelines for pain treatment research
- PMID: 25919472
- PMCID: PMC4545735
- DOI: 10.1097/j.pain.0000000000000210
Transcranial magnetic stimulation of the brain: guidelines for pain treatment research
Abstract
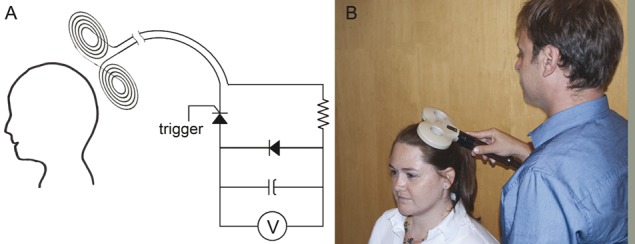
Recognizing that electrically stimulating the motor cortex could relieve chronic pain sparked development of noninvasive technologies. In transcranial magnetic stimulation (TMS), electromagnetic coils held against the scalp influence underlying cortical firing. Multiday repetitive transcranial magnetic stimulation (rTMS) can induce long-lasting, potentially therapeutic brain plasticity. Nearby ferromagnetic or electronic implants are contraindications. Adverse effects are minimal, primarily headaches. Single provoked seizures are very rare. Transcranial magnetic stimulation devices are marketed for depression and migraine in the United States and for various indications elsewhere. Although multiple studies report that high-frequency rTMS of the motor cortex reduces neuropathic pain, their quality has been insufficient to support Food and Drug Administration application. Harvard's Radcliffe Institute therefore sponsored a workshop to solicit advice from experts in TMS, pain research, and clinical trials. They recommended that researchers standardize and document all TMS parameters and improve strategies for sham and double blinding. Subjects should have common well-characterized pain conditions amenable to motor cortex rTMS and studies should be adequately powered. They recommended standardized assessment tools (eg, NIH's PROMIS) plus validated condition-specific instruments and consensus-recommended metrics (eg, IMMPACT). Outcomes should include pain intensity and qualities, patient and clinician impression of change, and proportions achieving 30% and 50% pain relief. Secondary outcomes could include function, mood, sleep, and/or quality of life. Minimum required elements include sample sources, sizes, and demographics, recruitment methods, inclusion and exclusion criteria, baseline and posttreatment means and SD, adverse effects, safety concerns, discontinuations, and medication-usage records. Outcomes should be monitored for at least 3 months after initiation with prespecified statistical analyses. Multigroup collaborations or registry studies may be needed for pivotal trials.
Conflict of interest statement
Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article.
Figures
Comment in
-
Repetitive transcranial magnetic stimulation for pain: is it too early to standardise repetitive transcranial magnetic stimulation protocols?Pain. 2016 May;157(5):1174-1175. doi: 10.1097/j.pain.0000000000000503. Pain. 2016. PMID: 27081840 No abstract available.
-
Reply.Pain. 2016 May;157(5):1175-1176. doi: 10.1097/j.pain.0000000000000504. Pain. 2016. PMID: 27081841 No abstract available.
References
-
- Available at: http://www.fda.gov/MedicalDevices/DeviceRegulationandGuidance/GuidanceDo..., 2015.
-
- Available at: http://www.accessdata.fda.gov/cdrh_docs/pdf12/K122288.pdf, 2015.
-
- Available at: http://www.fda.gov/AboutFDA/CentersOffices/OfficeofMedicalProductsandTob..., 2015.
-
- Available at: http://www.fda.gov/downloads/MedicalDevices/DeviceRegulationandGuidance/..., 2015.
-
- Ahdab R, Ayache SS, Brugieres P, Goujon C, Lefaucheur JP. Comparison of “standard” and “navigated” procedures of TMS coil positioning over motor, premotor and prefrontal targets in patients with chronic pain and depression. Neurophysiol Clin 2010;40:27–36. - PubMed
Publication types
MeSH terms
Grants and funding
- R21 NS085491/NS/NINDS NIH HHS/United States
- K23 NS083741/NS/NINDS NIH HHS/United States
- R21 NS082870/NS/NINDS NIH HHS/United States
- NS38493/NS/NINDS NIH HHS/United States
- R21 MH099196/MH/NIMH NIH HHS/United States
- R01NS073601/NS/NINDS NIH HHS/United States
- K24 NS059892/NS/NINDS NIH HHS/United States
- UL1 RR025758/RR/NCRR NIH HHS/United States
- K23NS083741/NS/NINDS NIH HHS/United States
- R01 NS038493/NS/NINDS NIH HHS/United States
- R56 NS038493/NS/NINDS NIH HHS/United States
- U01 NS077179/NS/NINDS NIH HHS/United States
- R21 HD07616/HD/NICHD NIH HHS/United States
- R01 NS073601/NS/NINDS NIH HHS/United States
- K24NS059892/NS/NINDS NIH HHS/United States
- ImNIH/Intramural NIH HHS/United States
- R01HD069776/HD/NICHD NIH HHS/United States
- R01 HD069776/HD/NICHD NIH HHS/United States
- U01NS077179/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
