

Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial
- PMID: 25919527
- PMCID: PMC4527523
- DOI: 10.1001/jama.2015.3474
Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial
Abstract
Importance: Opioid-dependent patients often use the emergency department (ED) for medical care.
Objective: To test the efficacy of 3 interventions for opioid dependence: (1) screening and referral to treatment (referral); (2) screening, brief intervention, and facilitated referral to community-based treatment services (brief intervention); and (3) screening, brief intervention, ED-initiated treatment with buprenorphine/naloxone, and referral to primary care for 10-week follow-up (buprenorphine).
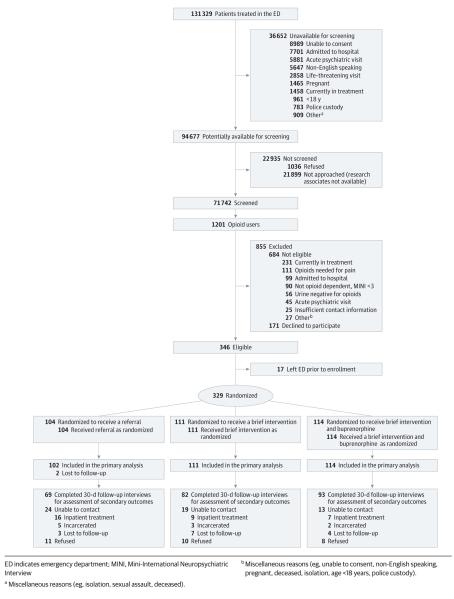
Design, setting, and participants: A randomized clinical trial involving 329 opioid-dependent patients who were treated at an urban teaching hospital ED from April 7, 2009, through June 25, 2013.
Interventions: After screening, 104 patients were randomized to the referral group, 111 to the brief intervention group, and 114 to the buprenorphine treatment group.
Main outcomes and measures: Enrollment in and receiving addiction treatment 30 days after randomization was the primary outcome. Self-reported days of illicit opioid use, urine testing for illicit opioids, human immunodeficiency virus (HIV) risk, and use of addiction treatment services were the secondary outcomes.
Results: Seventy-eight percent of patients in the buprenorphine group (89 of 114 [95% CI, 70%-85%]) vs 37% in the referral group (38 of 102 [95% CI, 28%-47%]) and 45% in the brief intervention group (50 of 111 [95% CI, 36%-54%]) were engaged in addiction treatment on the 30th day after randomization (P < .001). The buprenorphine group reduced the number of days of illicit opioid use per week from 5.4 days (95% CI, 5.1-5.7) to 0.9 days (95% CI, 0.5-1.3) vs a reduction from 5.4 days (95% CI, 5.1-5.7) to 2.3 days (95% CI, 1.7-3.0) in the referral group and from 5.6 days (95% CI, 5.3-5.9) to 2.4 days (95% CI, 1.8-3.0) in the brief intervention group (P < .001 for both time and intervention effects; P = .02 for the interaction effect). The rates of urine samples that tested negative for opioids did not differ statistically across groups, with 53.8% (95% CI, 42%-65%) in the referral group, 42.9% (95% CI, 31%-55%) in the brief intervention group, and 57.6% (95% CI, 47%-68%) in the buprenorphine group (P = .17). There were no statistically significant differences in HIV risk across groups (P = .66). Eleven percent of patients in the buprenorphine group (95% CI, 6%-19%) used inpatient addiction treatment services, whereas 37% in the referral group (95% CI, 27%-48%) and 35% in the brief intervention group (95% CI, 25%-37%) used inpatient addiction treatment services (P < .001).
Conclusions and relevance: Among opioid-dependent patients, ED-initiated buprenorphine treatment vs brief intervention and referral significantly increased engagement in addiction treatment, reduced self-reported illicit opioid use, and decreased use of inpatient addiction treatment services but did not significantly decrease the rates of urine samples that tested positive for opioids or of HIV risk. These findings require replication in other centers before widespread adoption.
Trial registration: clinicaltrials.gov Identifier: NCT00913770.
Figures
Comment in
-
Opioid Dependence Treatment in the Emergency Department.JAMA. 2015 Aug 25;314(8):834-5. doi: 10.1001/jama.2015.8519. JAMA. 2015. PMID: 26305656 No abstract available.
-
Opioid Dependence Treatment in the Emergency Department--Reply.JAMA. 2015 Aug 25;314(8):835. doi: 10.1001/jama.2015.8527. JAMA. 2015. PMID: 26305657 No abstract available.
References
-
- Centers for Disease Control and Prevention (CDC) Emergency department visits involving nonmedical use of selected prescription drugs—United States, 2004-2008. MMWR Morb Mortal Wkly Rep. 2010;59(23):705–709. - PubMed
-
- Centers for Disease Control and Prevention (CDC) CDC grand rounds: prescription drug overdoses—a US epidemic. MMWR Morb Mortal Wkly Rep. 2012;61(1):10–13. - PubMed
-
- Gowing L, Farrell MF, Bornemann R, Sullivan LE, Ali R. Oral substitution treatment of injecting opioid users for prevention of HIV infection. Cochrane Database Syst Rev. 2011;8(8):CD004145. - PubMed
-
- Guidelines for the Psychosocially Assisted Pharmacological Treatment of Opioid Dependence. World Health Organization; Geneva, Switzerland: 2009. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
