

Liver cancer: Approaching a personalized care
- PMID: 25920083
- PMCID: PMC4520430
- DOI: 10.1016/j.jhep.2015.02.007
Liver cancer: Approaching a personalized care
Abstract
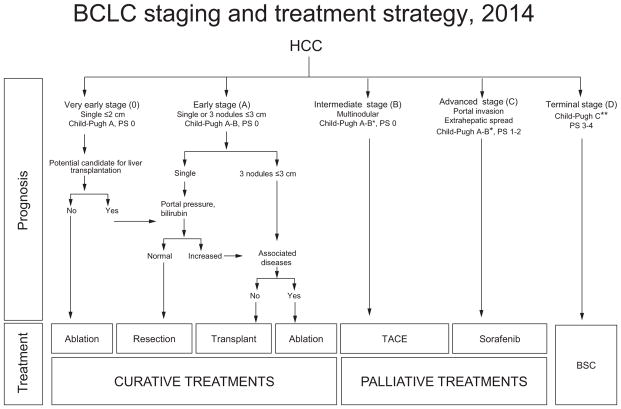
The knowledge and understanding of all aspects of liver cancer [this including hepatocellular carcinoma (HCC) and intrahepatic cholangiocarcinoma (iCCA)] have experienced a major improvement in the last decades. New laboratory technologies have identified several molecular abnormalities that, at the very end, should provide an accurate stratification and optimal treatment of patients diagnosed with liver cancer. The seminal discovery of the TP53 hotspot mutation [1,2] was an initial landmark step for the future classification and treatment decision using conventional clinical criteria blended with molecular data. At the same time, the development of ultrasound, computed tomography (CT) and magnetic resonance (MR) has been instrumental for earlier diagnosis, accurate staging and treatment advances. Several treatment options with proven survival benefit if properly applied are now available. Major highlights include: i) acceptance of liver transplantation for HCC if within the Milan criteria [3], ii) recognition of ablation as a potentially curative option [4,5], iii) proof of benefit of chemoembolization (TACE), [6] and iv) incorporation of sorafenib as an effective systemic therapy [7]. These options are part of the widely endorsed BCLC staging and treatment model (Fig. 1) [8,9]. This is clinically useful and it will certainly keep evolving to accommodate new scientific evidence.
This review summarises the data which are the basis for the current recommendations for clinical practice, while simultaneously exposes the areas where more research is needed to fulfil the still unmet needs (Table 1).
Keywords: HCC; Liver cancer; Personalised treatment; Profiling; iCCA.
Conflict of interest statement
J Bruix has received research support from Bayer HealthCare Pharmaceuticals and consulting fees from Bayer HealthCare Pharmaceuticals, Onyx Pharmaceuticals, Arqule, Bristol-Myers-Squibb, BTG, Imclone-Lilly, Novartis, Terumo, Roche, Kowa and BioAlliance. GJ Gores has received consultancy fees from Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb, Chugai, Daiichi Sanyo, Delcath, Genentech, and Generon. Josep M. Llovet has received research support from Bayer Healthcare Pharmaceuticals, Bristol Myers Squibb and Boehringer-Ingelheim, abd consutancy fees from Bayer Healthcare Pharmaceuticals, Bristol Myers Squibb, Boehringer-Ingelheim, Lilly Pharmaceuticals, Celsion, Biocompatibles, Novartis, GlaxoSmithKline and Blueprint Medicines. V Mazzaferro declares conflict of interest due to consultancy with Bayer and BTG Biocompatibles having received consulting fees from the two. KH Han has received consulting fees from Eisai Pharmaceuticals and KOWA.
Figures
References
-
- Bressac B, Kew M, Wands J, Ozturk M. Selective G to T mutations of p53 gene in hepatocellular carcinoma from southern Africa. Nature. 1991;350:429–431. http://dx.doi.org/10.1038/350429a0. - DOI - PubMed
-
- Hsu IC, Metcalf RA, Sun T, Welsh JA, Wang NJ, Harris CC. Mutational hotspot in the p53 gene in human hepatocellular carcinomas. Nature. 1991;350:427–428. http://dx.doi.org/10.1038/350427a0. - DOI - PubMed
-
- Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334:693–699. - PubMed
-
- EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56:908–943. http://dx.doi.org/10.1016/j.jhep.2011.12.001, pii: S0168-8278(11)00873-7. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
