

Trends in the management and burden of alcoholic liver disease
- PMID: 25920088
- PMCID: PMC5013530
- DOI: 10.1016/j.jhep.2015.03.006
Trends in the management and burden of alcoholic liver disease
Abstract
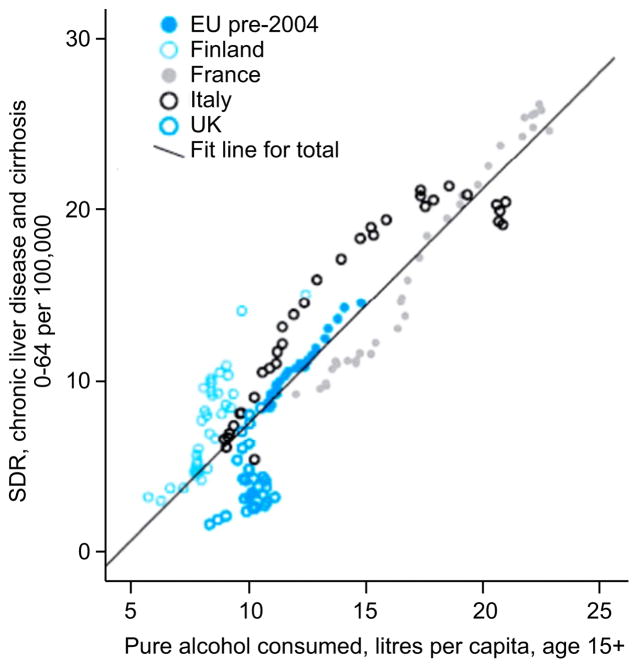
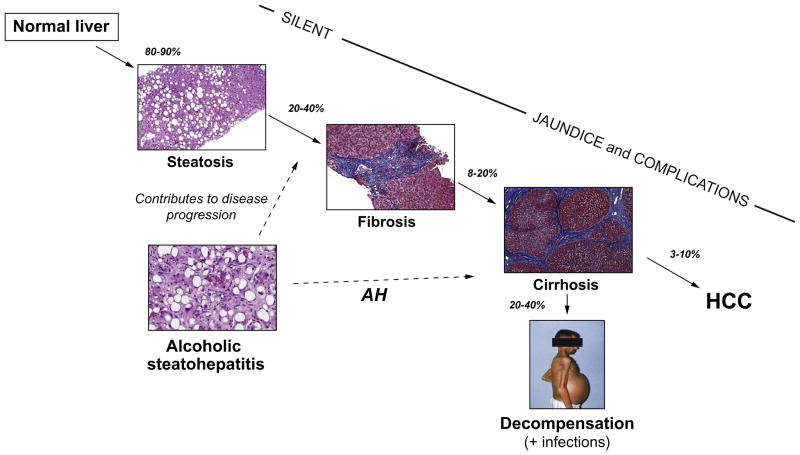
Alcoholic liver disease (ALD) is the most prevalent cause of advanced liver disease in Europe and is the leading cause of death among adults with excessive alcohol consumption. There is a dose-response relationship between the amount of alcohol consumed and the risk of ALD. The relative risk of cirrhosis increases in subjects who consume more than 25 g/day. The burden of alcohol-attributable liver cirrhosis and liver cancer is high and is entirely preventable. Health agencies should develop population-based policies to reduce the prevalence of harmful and/or hazardous alcohol consumption and foster research in this field to provide new diagnostic and therapeutic tools. Disease progression of patients with ALD is heavily influenced by both genetic and environmental factors. Non-invasive methods for the diagnosis of fibrosis have opened new perspectives in the early detection of advanced ALD in asymptomatic patients. Alcoholic hepatitis, the most severe form of ALD, carries a high short-term mortality (around 30-50% at 3 months). Corticosteroids improve short-term survival in patients with severe alcoholic hepatitis but duration of therapy should be adapted to early response. Liver transplantation is the best option for patients with severe liver dysfunction. However, alcohol relapse after transplantation remains a critical issue and drinking habits of transplanted patients need to be routinely screened.
Keywords: Alcoholic hepatitis; Burden of alcoholic liver disease; Cirrhosis; Liver transplantation; Natural history; Non-invasive diagnosis.
Copyright © 2015. Published by Elsevier B.V.
Conflict of interest statement
Ramon Bataller has provided consulting services to Sandhill Scientific. Philippe Mathurin has nothing to disclose.
Figures

References
-
- Rehm J, Room R, Monteiro M, et al. Alcohol as a risk factor for global burden of disease. Eur Addict Res. 2003;9:157–164. - PubMed
-
- European Association for the Study of Liver. EASL clinical practical guidelines: management of alcoholic liver disease. J Hepatol. 2012;57:399–420. - PubMed
-
- Askgaard G, Gronbaek M, Kjaer MS, et al. Alcohol drinking pattern and risk of alcoholic liver cirrhosis: a prospective cohort study. J Hepatol. 2015 http://dx.doi.org/10.1016/j.jhep.2014.12.005, in press. - DOI - PubMed
-
- Zakhari S, Li T. Determinants of alcohol use and abuse: impact of quantity and frequency patterns on liver disease. Hepatology. 2007;46:2032–2039. - PubMed
-
- Pincock S. Binge drinking on rise in UK and elsewhere. Lancet. 2003;362:1126–1127. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
