

Epileptogenic zone localization using magnetoencephalography predicts seizure freedom in epilepsy surgery
- PMID: 25921215
- PMCID: PMC4457690
- DOI: 10.1111/epi.13002
Epileptogenic zone localization using magnetoencephalography predicts seizure freedom in epilepsy surgery
Abstract
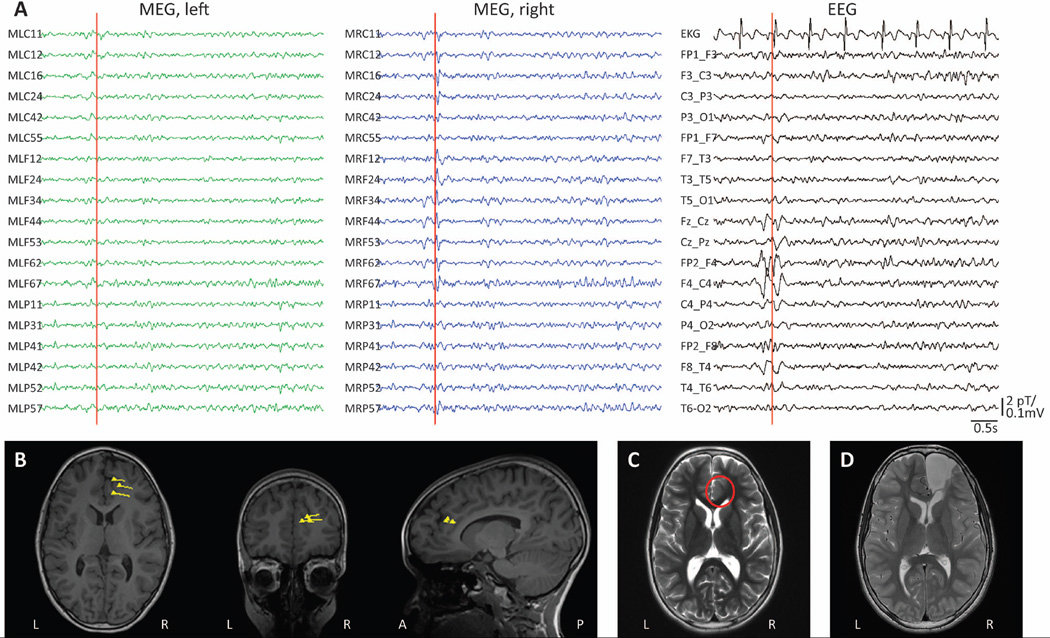
Objective: The efficacy of epilepsy surgery depends critically upon successful localization of the epileptogenic zone. Magnetoencephalography (MEG) enables noninvasive detection of interictal spike activity in epilepsy, which can then be localized in three dimensions using magnetic source imaging (MSI) techniques. However, the clinical value of MEG in the presurgical epilepsy evaluation is not fully understood, as studies to date are limited by either a lack of long-term seizure outcomes or small sample size.
Methods: We performed a retrospective cohort study of patients with focal epilepsy who received MEG for interictal spike mapping followed by surgical resection at our institution.
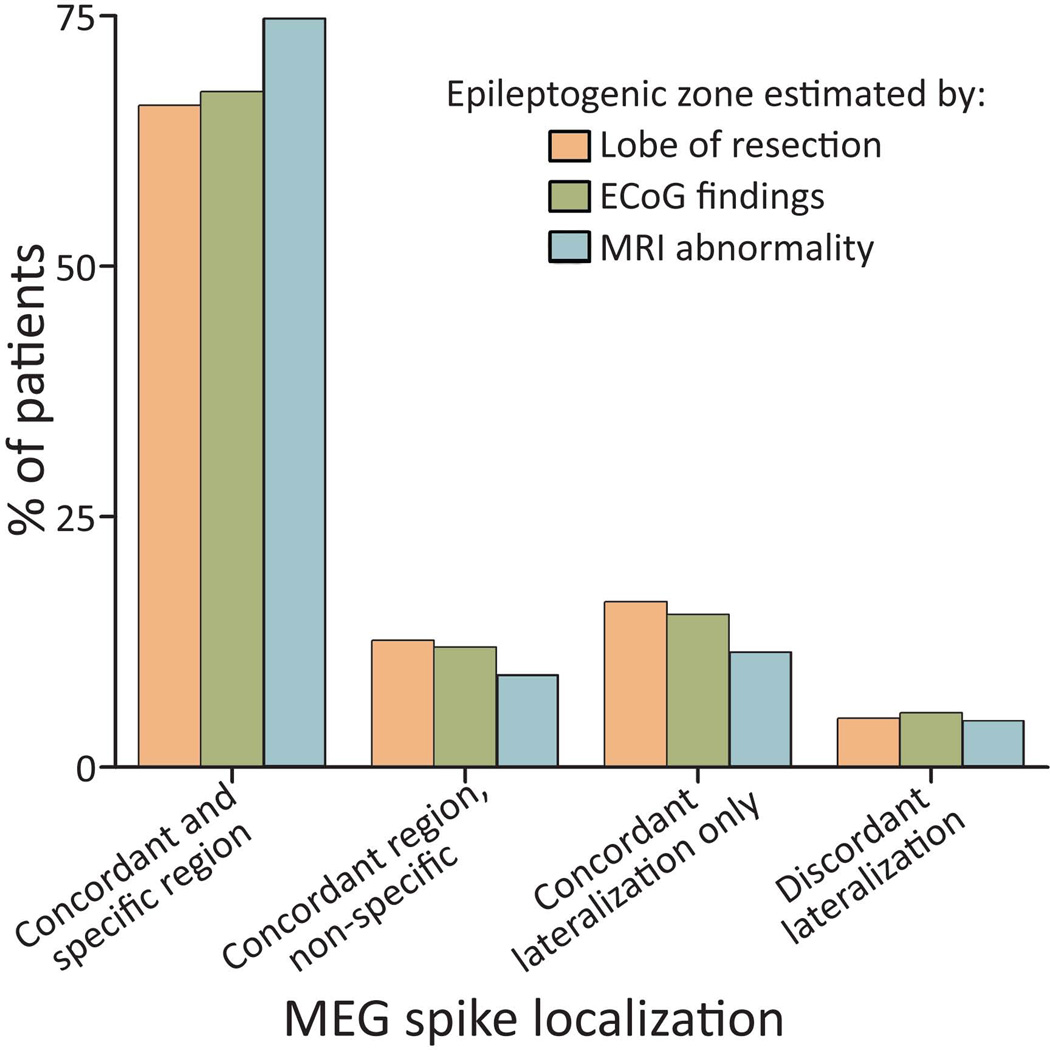
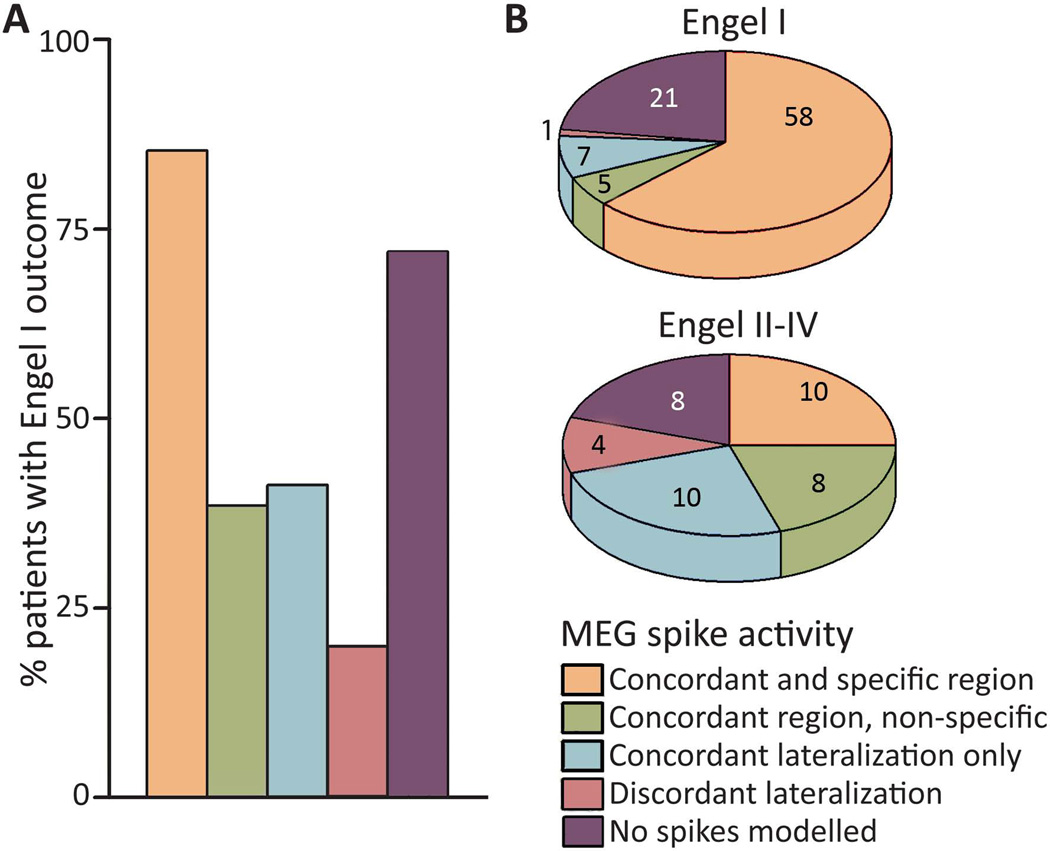
Results: We studied 132 surgical patients, with mean postoperative follow-up of 3.6 years (minimum 1 year). Dipole source modeling was successful in 103 patients (78%), whereas no interictal spikes were seen in others. Among patients with successful dipole modeling, MEG findings were concordant with and specific to the following: (1) the region of resection in 66% of patients, (2) invasive electrocorticography (ECoG) findings in 67% of individuals, and (3) the magnetic resonance imaging (MRI) abnormality in 74% of cases. MEG showed discordant lateralization in ~5% of cases. After surgery, 70% of all patients achieved seizure freedom (Engel class I outcome). Whereas 85% of patients with concordant and specific MEG findings became seizure-free, this outcome was achieved by only 37% of individuals with MEG findings that were nonspecific to or discordant with the region of resection (χ(2) = 26.4, p < 0.001). MEG reliability was comparable in patients with or without localized scalp electroencephalography (EEG), and overall, localizing MEG findings predicted seizure freedom with an odds ratio of 5.11 (95% confidence interval [CI] 2.23-11.8).
Significance: MEG is a valuable tool for noninvasive interictal spike mapping in epilepsy surgery, including patients with nonlocalized findings receiving long-term EEG monitoring, and localization of the epileptogenic zone using MEG is associated with improved seizure outcomes.
Keywords: Epilepsy surgery; Epileptogenic zone; Interictal spike; Magnetic source imaging; Magnetoencephalography.
Wiley Periodicals, Inc. © 2015 International League Against Epilepsy.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Cascino GD. When drugs and surgery don't work. Epilepsia. 2008;49(Suppl 9):79–84. - PubMed
-
- Englot DJ, Lee AT, Tsai C, et al. Seizure types and frequency in patients who "fail" temporal lobectomy for intractable epilepsy. Neurosurgery. 2013;73:838–844. - PubMed
-
- Spencer S, Huh L. Outcomes of epilepsy surgery in adults and children. Lancet Neurol. 2008;7:525–537. - PubMed
-
- Englot DJ, Breshears JD, Sun PP, et al. Seizure outcomes after resective surgery for extra-temporal lobe epilepsy in pediatric patients. J Neurosurg Pediatr. 2013;12:126–133. - PubMed
-
- Englot DJ, Rolston JD, Wang DD, et al. Seizure outcomes after temporal lobectomy in pediatric patients. J Neurosurg Pediatr. 2013;12:134–141. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
