

Effect of Amitriptyline and Escitalopram on Functional Dyspepsia: A Multicenter, Randomized Controlled Study
- PMID: 25921377
- PMCID: PMC4516571
- DOI: 10.1053/j.gastro.2015.04.020
Effect of Amitriptyline and Escitalopram on Functional Dyspepsia: A Multicenter, Randomized Controlled Study
Abstract
Background & aims: Antidepressants are frequently prescribed to treat functional dyspepsia (FD), a common disorder characterized by upper abdominal symptoms, including discomfort or postprandial fullness. However, there is little evidence of the efficacy of these drugs in patients with FD. We performed a randomized, double-blind, placebo-controlled trial to evaluate the effects of antidepressant therapy on symptoms, gastric emptying (GE), and meal-induced satiety in patients with FD.
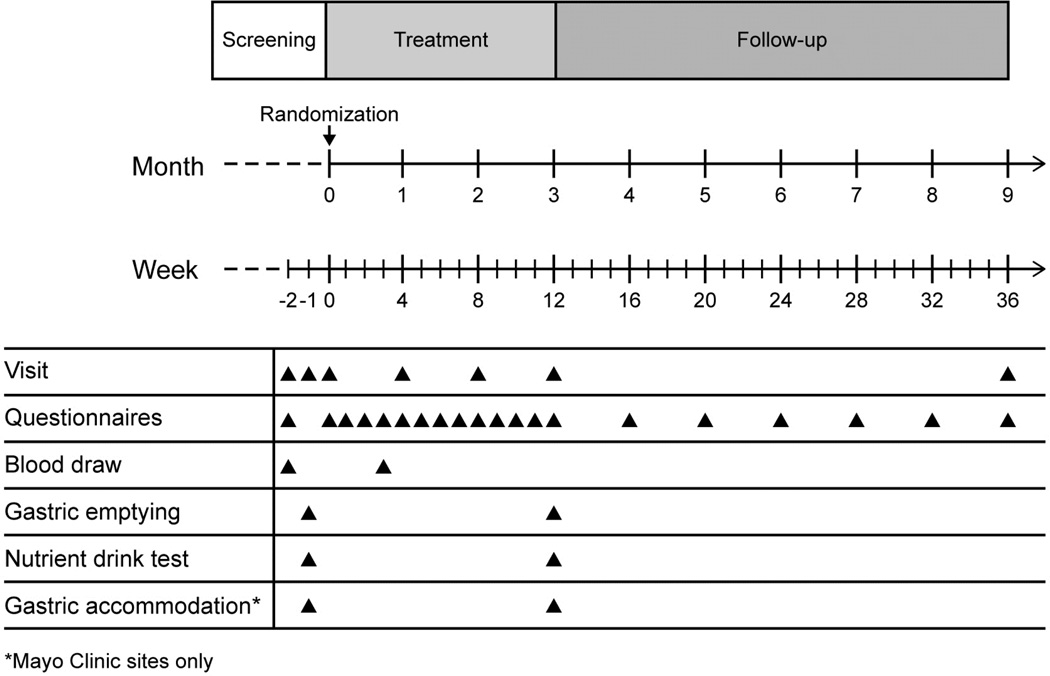
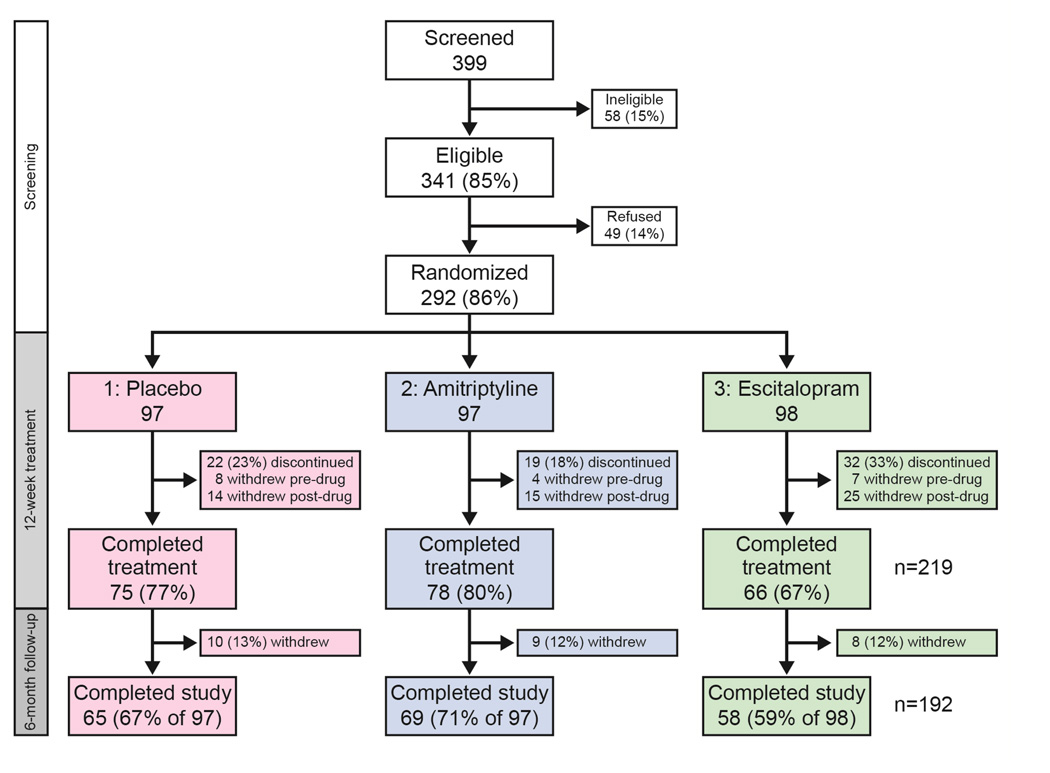
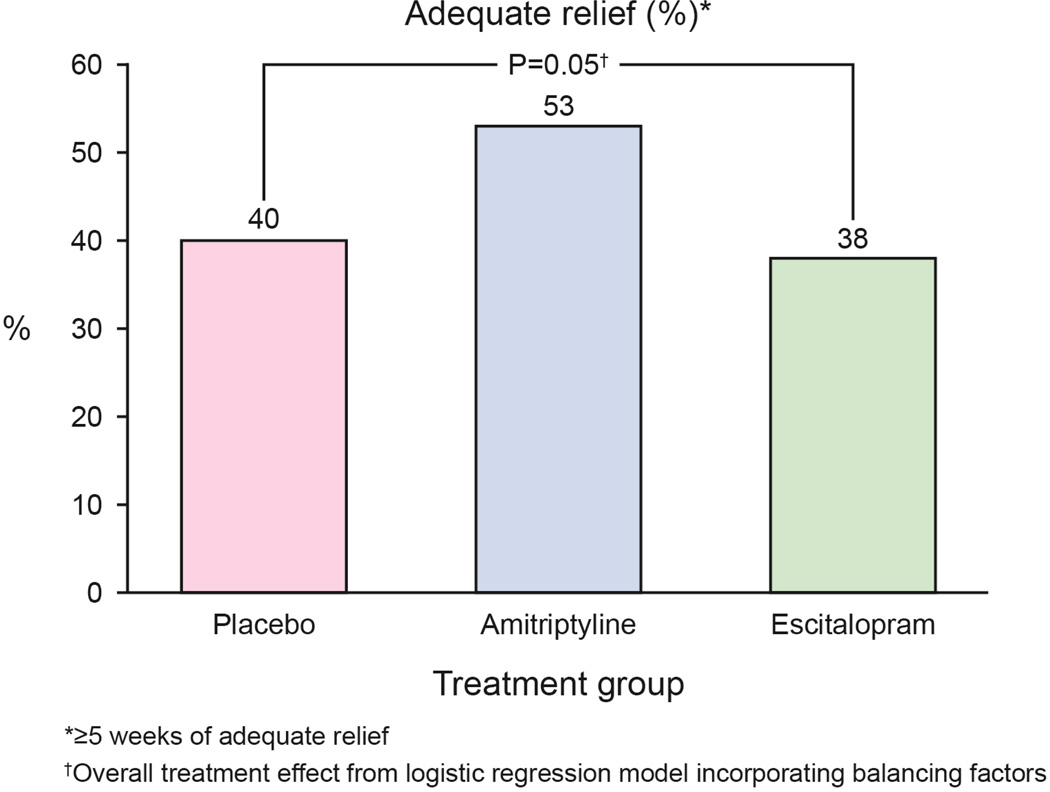
Methods: We performed a study at 8 North American sites of patients who met the Rome II criteria for FD and did not have depression or use antidepressants. Patients (n = 292; 44 ± 15 years old, 75% were female, 70% with dysmotility-like FD, and 30% with ulcer-like FD) were randomly assigned to groups given placebo, 50 mg amitriptyline, or 10 mg escitalopram for 10 weeks. The primary end point was adequate relief of FD symptoms for ≥5 weeks of the last 10 weeks (of 12). Secondary end points included GE time, maximum tolerated volume in Nutrient Drink Test, and FD-related quality of life.
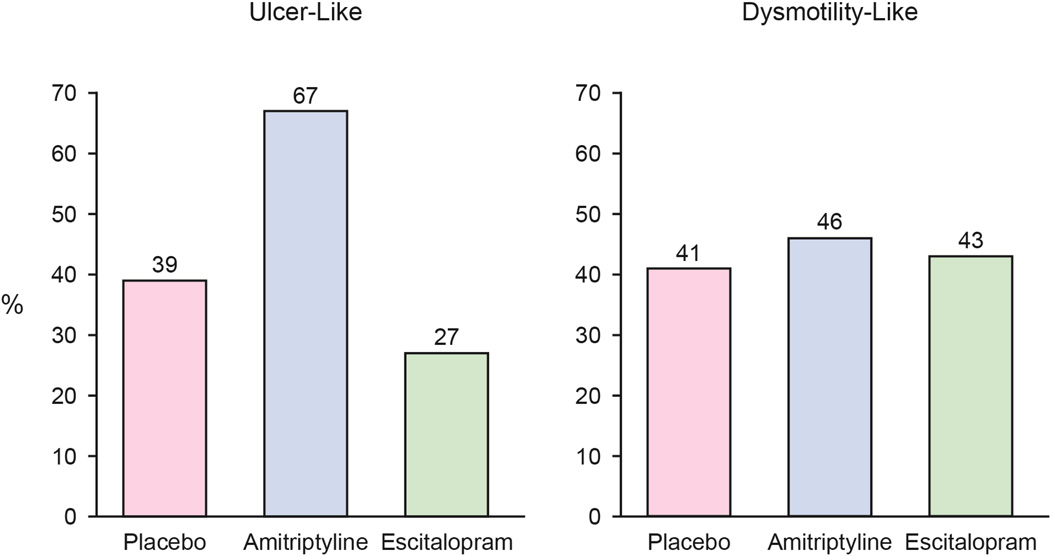
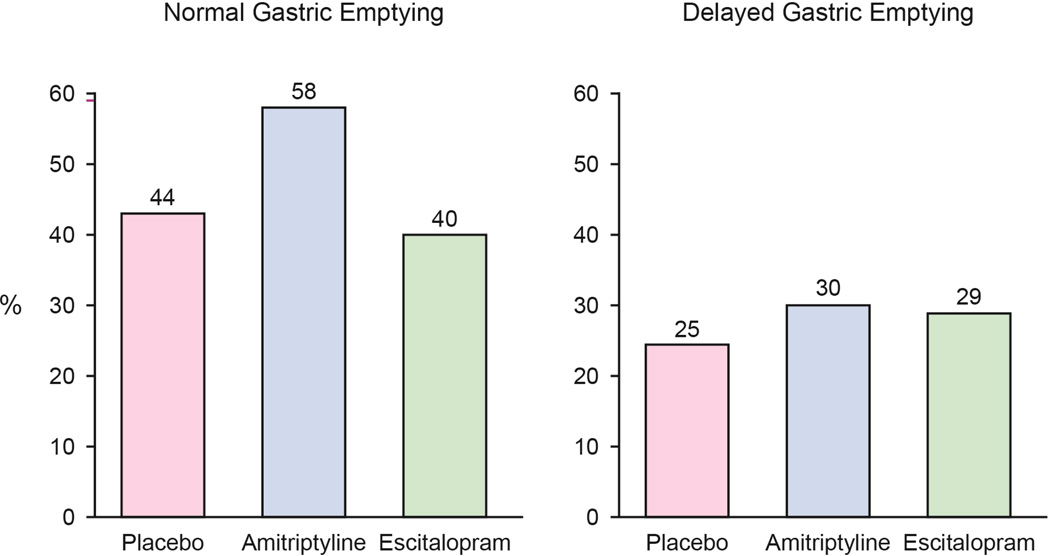
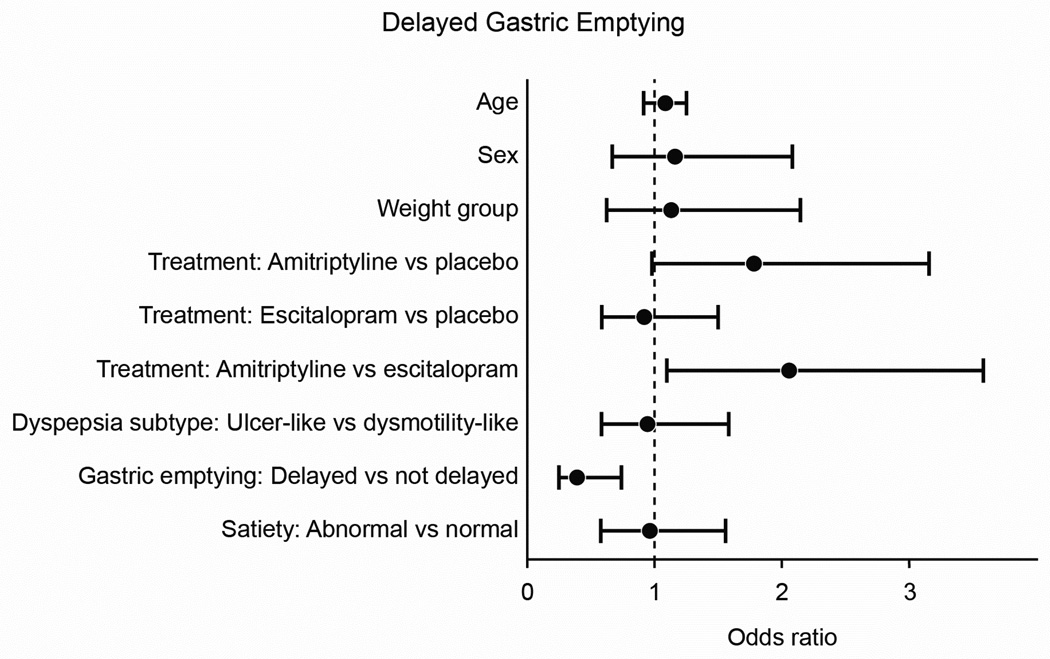
Results: An adequate relief response was reported by 39 subjects given placebo (40%), 51 given amitriptyline (53%), and 37 given escitalopram (38%) (P = .05, after treatment, adjusted for baseline balancing factors including all subjects). Subjects with ulcer-like FD given amitriptyline were >3-fold more likely to report adequate relief than those given placebo (odds ratio = 3.1; 95% confidence interval: 1.1-9.0). Neither amitriptyline nor escitalopram appeared to affect GE or meal-induced satiety after the 10-week period in any group. Subjects with delayed GE were less likely to report adequate relief than subjects with normal GE (odds ratio = 0.4; 95% confidence interval: 0.2-0.8). Both antidepressants improved overall quality of life.
Conclusions: Amitriptyline, but not escitalopram, appears to benefit some patients with FD, particularly those with ulcer-like (painful) FD. Patients with delayed GE do not respond to these drugs. ClinicalTrials.gov ID: NCT00248651.
Keywords: Abdominal Pain; Antidepressant; Functional Dyspepsia; Functional Gastrointestinal Disorder.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Amitriptyline for Functional Dyspepsia: Importance of Symptom Profile and Making a Case for Gastric Emptying Testing.Gastroenterology. 2015 Aug;149(2):270-2. doi: 10.1053/j.gastro.2015.06.017. Epub 2015 Jun 25. Gastroenterology. 2015. PMID: 26116797 No abstract available.
-
Effect of Amitriptyline and Escitalopram on Functional Dyspepsia.Gastroenterology. 2016 Feb;150(2):532. doi: 10.1053/j.gastro.2015.10.051. Epub 2015 Dec 21. Gastroenterology. 2016. PMID: 26718171 No abstract available.
-
Reply.Gastroenterology. 2016 Feb;150(2):532-3. doi: 10.1053/j.gastro.2015.12.029. Epub 2015 Dec 21. Gastroenterology. 2016. PMID: 26718175 No abstract available.
-
[Effect of Amitriptyline in Patients with Functional Dyspepsia].Korean J Gastroenterol. 2015 Oct;66(4):245-7. doi: 10.4166/kjg.2015.66.4.245. Korean J Gastroenterol. 2015. PMID: 26793809 Korean. No abstract available.
References
-
- Tack J, Talley NJ. Functional dyspepsia--symptoms, definitions and validity of the Rome III criteria. Nat Rev Gastroenterol Hepatol. 2013;10:134–141. - PubMed
-
- Talley NJ, Walker MM, Aro P, et al. Non-ulcer dyspepsia and duodenal eosinophilia: an adult endoscopic population-based case-control study. Clin Gastroenterol Hepatol. 2007;5:1175–1183. - PubMed
-
- Camilleri M, Dubois D, Coulie B, et al. Prevalence and socioeconomic impact of upper gastrointestinal disorders in the United States: results of the US Upper Gastrointestinal Study. Clin Gastroenterol Hepatol. 2005;3:543–552. - PubMed
-
- Tack J, Caenepeel P, Fischler B, et al. Symptoms associated with hypersensitivity to gastric distention in functional dyspepsia. Gastroenterology. 2001;121:526–535. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
