

Therapy in stable chronic obstructive pulmonary disease patients with pulmonary hypertension: a systematic review and meta-analysis
- PMID: 25922708
- PMCID: PMC4387388
- DOI: 10.3978/j.issn.2072-1439.2015.02.08
Therapy in stable chronic obstructive pulmonary disease patients with pulmonary hypertension: a systematic review and meta-analysis
Abstract
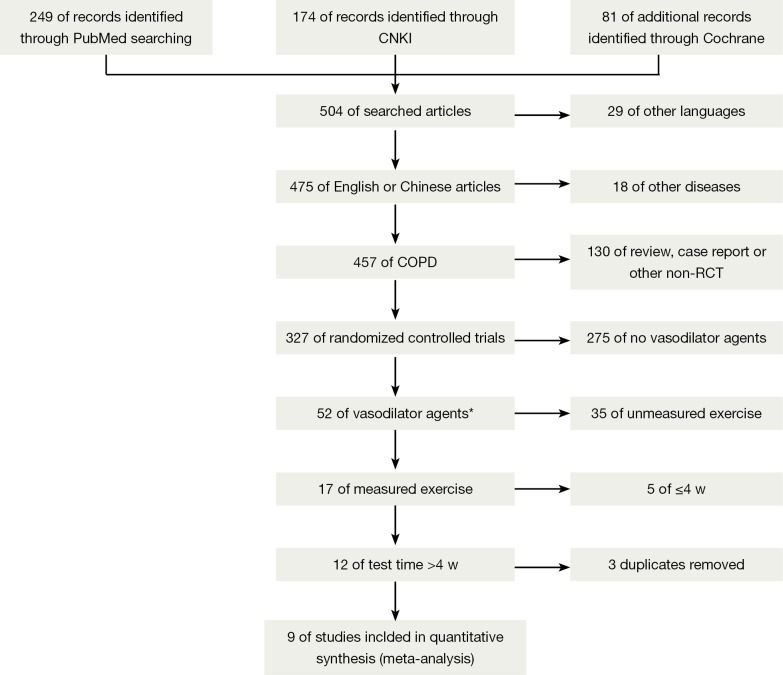
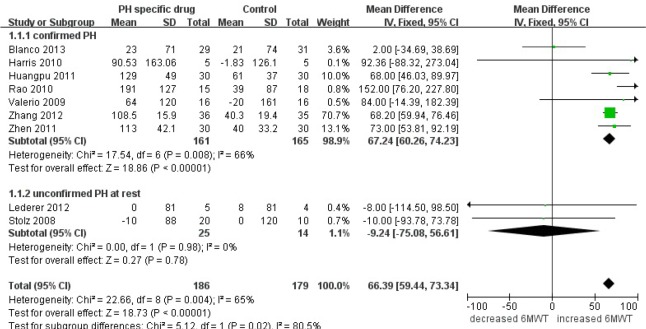
Pulmonary hypertension (PH) is a common complication of chronic obstructive pulmonary disease (COPD) without effective drugs to treat. We conducted a systematic review and meta-analysis in order to evaluate whether PH specific therapies were effective for stable COPD patients. Data were extracted from PubMed, Cochrane Central Register of Controlled Trials and China Knowledge Resource Integrated Database. Randomized controlled trials (RCTs) with PH specific therapy treated more than 4 weeks in COPD were selected. The main outcome was exercise capacity; meanwhile pulmonary arterial pressure (PAP), hypoxemia and health related life quality were also measured. We included nine trials involving 365 subjects, among which two were treated with bosentan and seven with sildenafil. The study time varied from 4 weeks to 18 months and mostly it was 12 weeks. In a pooled analysis of nine trials, exercise capacity of COPD patients was improved by PH-specific therapy [mean difference (MD) 66.39 m, 95% confidence intervals (CI): 59.44-73.34]. COPD with severe PH (mean PAP >35 mmHg by right heart catheterization or systolic PAP >50 mmHg by echocardiography) improved the exercise capacity (MD 67.24 m, 95% CI: 60.26-74.23), but COPD without PH at rest did not (MD -9.24 m, 95% CI: -75.08 to 56.31). Meanwhile PAP was decreased (MD -9.02 mmHg, 95% CI: -10.71 to -7.34 mmHg). Although hypoxemia and life quality were not improved, the dyspnea was alleviated or at least not aggravated (Borg dyspnea index, MD -0.86, 95% CI: -1.86 to 0.14). In conclusion, PH specific drugs (especially sildenafil) could improve exercise capacity and decrease PAP in COPD patients with severe PH.
Keywords: Chronic obstructive pulmonary disease (COPD); exercise capacity; pulmonary arterial pressure (PAP); pulmonary hypertension (PH); treatment.
Figures






References
-
- O’Donnell DE, Banzett RB, Carrieri-Kohlman V, et al. Pathophysiology of dyspnea in chronic obstructive pulmonary disease: a roundtable. Proc Am Thorac Soc 2007;4:145-68. - PubMed
-
- Simonneau G, Gatzoulis MA, Adatia I, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol 2013;62:D34-41. - PubMed
-
- Kessler R, Faller M, Weitzenblum E, et al. “Natural history” of pulmonary hypertension in a series of 131 patients with chronic obstructive lung disease. Am J Respir Crit Care Med 2001;164:219-24. - PubMed
-
- Chaouat A, Bugnet AS, Kadaoui N, et al. Severe pulmonary hypertension and chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2005;172:189-94. - PubMed
-
- Andersen KH, Iversen M, Kjaergaard J, et al. Prevalence, predictors, and survival in pulmonary hypertension related to end-stage chronic obstructive pulmonary disease. J Heart Lung Transplant 2012;31:373-80. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials