

The efficacy and safety of prone positioning in adults patients with acute respiratory distress syndrome: a meta-analysis of randomized controlled trials
- PMID: 25922713
- PMCID: PMC4387391
- DOI: 10.3978/j.issn.2072-1439.2014.12.49
The efficacy and safety of prone positioning in adults patients with acute respiratory distress syndrome: a meta-analysis of randomized controlled trials
Abstract
Background: Prone positioning for acute respiratory distress syndrome (ARDS) has no impact on mortality despite significant improvements in oxygenation. However, a recent trial demonstrated reduced mortality rates in the prone position for severe ARDS. We evaluated effects of prone position duration and protective lung strategies on mortality rates in ARDS.
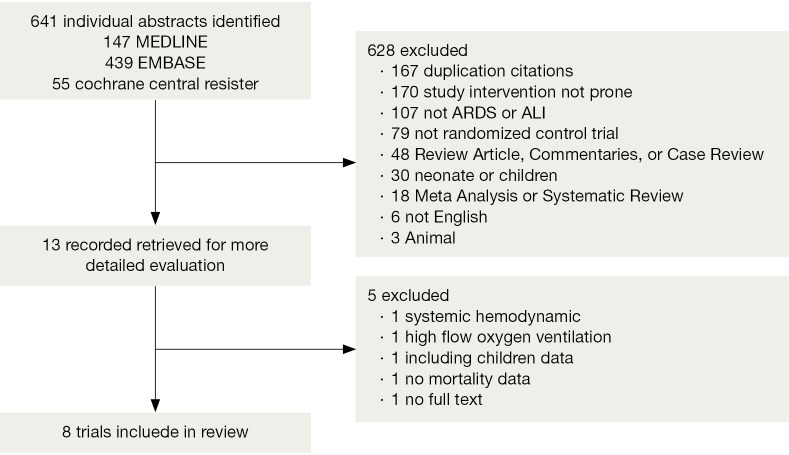
Methods: We extensively searched MEDLINE, EMBASE, and the Cochrane Central Register of Controlled Trials to identify randomized controlled trials (RCTs) reporting on prone positioning during acute respiratory failure in adults for inclusion in our meta-analysis.
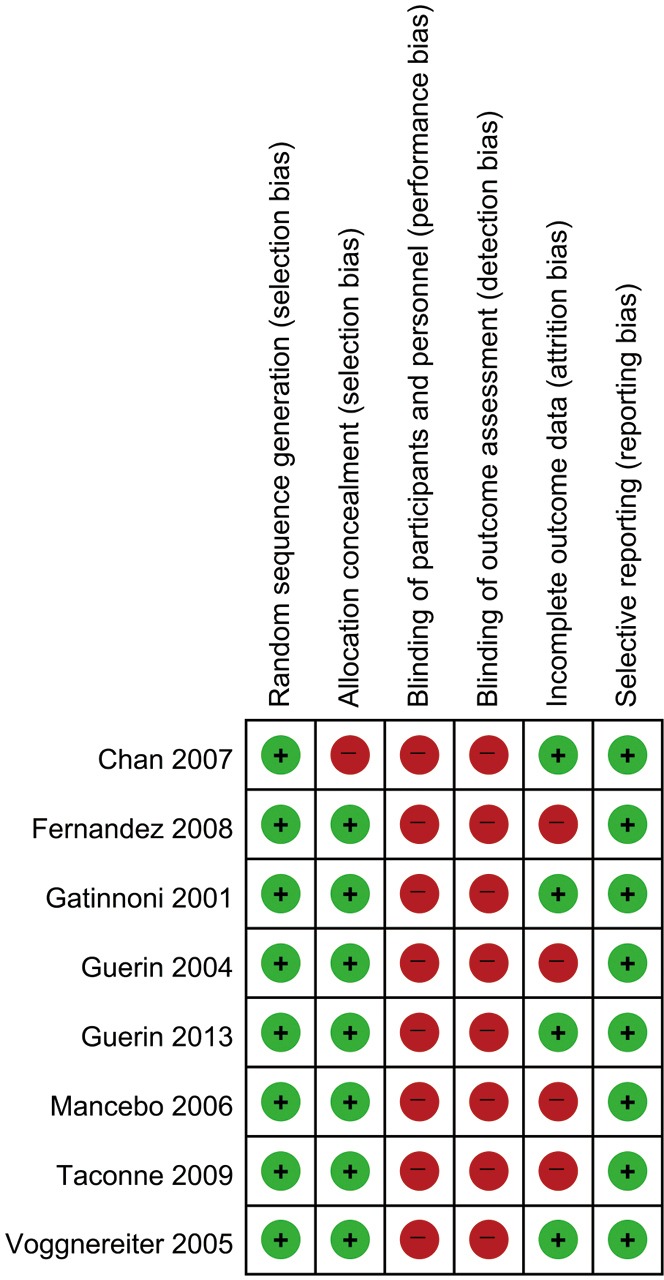
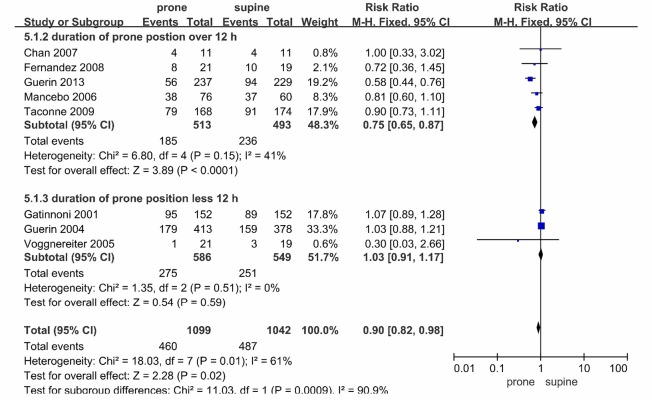
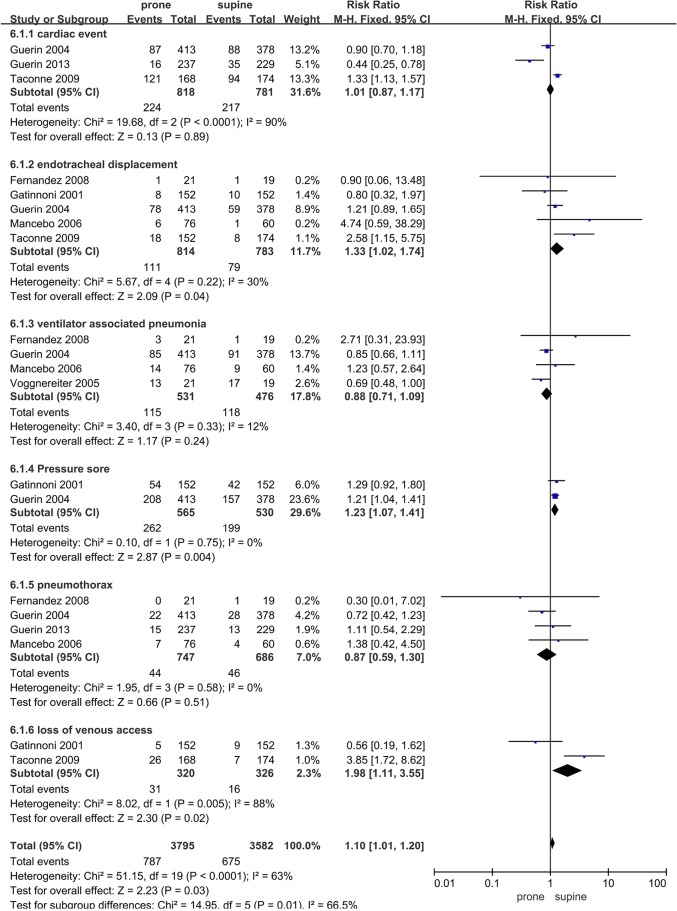
Results: Eight trials met our inclusion criteria, Totals of 1,099 and 1,042 patients were randomized to the prone and supine ventilation positions. The mortality rates associated with the prone and supine positions were 41% and 47% [risk ratio (RR), 0.90; 95% confidence interval (CI), 0.82-0.98, P=0.02], but the heterogeneity was moderate (P=0.01, I(2)=61%). In a subgroup analysis, the mortality rates for lung protective ventilation (RR 0.73, 95% CI, 0.62-0.86, P=0.0002) and duration of prone positioning >12 h (RR 0.75, 95% CI, 0.65-0.87, P<0.0001) were reduced in the prone position. Prone positioning was not associated with an increased incidence of cardiac events (RR 1.01, 95% CI, 0.87-1.17) or ventilator associated pneumonia (RR 0.88, 95% CI, 0.71-1.09), but it was associated with an increased incidence of pressure sores (RR 1.23, 95% CI, 1.07-1.41) and endotracheal dislocation (RR 1.33, 95% CI, 1.02-1.74).
Conclusions: Prone positioning tends to reduce the mortality rates in ARDS patients, especially when used in conjunction with a lung protective strategy and longer prone position durations. Prone positioning for ARDS patients should be prioritized over other invasive procedures because related life-threatening complications are rare. However, further additional randomized controlled design to study are required for confirm benefit of prone position in ARDS.
Keywords: Prone positioning; acute respiratory distress syndrome (ARDS); mortality.
Figures


References
-
- Villar J, Sulemanji D, Kacmarek RM. The acute respiratory distress syndrome: incidence and mortality, has it changed? Curr Opin Crit Care 2014;20:3-9. - PubMed
-
- Milberg JA, Davis DR, Steinberg KP, et al. Improved survival of patients with acute respiratory distress syndrome (ARDS): 1983-1993. JAMA 1995;273:306-9. - PubMed
-
- Bryan AC. Conference on the scientific basis of respiratory therapy. Pulmonary physiotherapy in the pediatric age group. Comments of a devil's advocate. Am Rev Respir Dis 1974;110:143-4. - PubMed
-
- Blanch L, Mancebo J, Perez M, et al. Short-term effects of prone position in critically ill patients with acute respiratory distress syndrome. Intensive Care Med 1997;23:1033-9. - PubMed
-
- Chatte G, Sab JM, Dubois JM, et al. Prone position in mechanically ventilated patients with severe acute respiratory failure. Am J Respir Crit Care Med 1997;155:473-8. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous