

Repetitive transcranial magnetic stimulation in cervical dystonia: effect of site and repetition in a randomized pilot trial
- PMID: 25923718
- PMCID: PMC4414555
- DOI: 10.1371/journal.pone.0124937
Repetitive transcranial magnetic stimulation in cervical dystonia: effect of site and repetition in a randomized pilot trial
Abstract
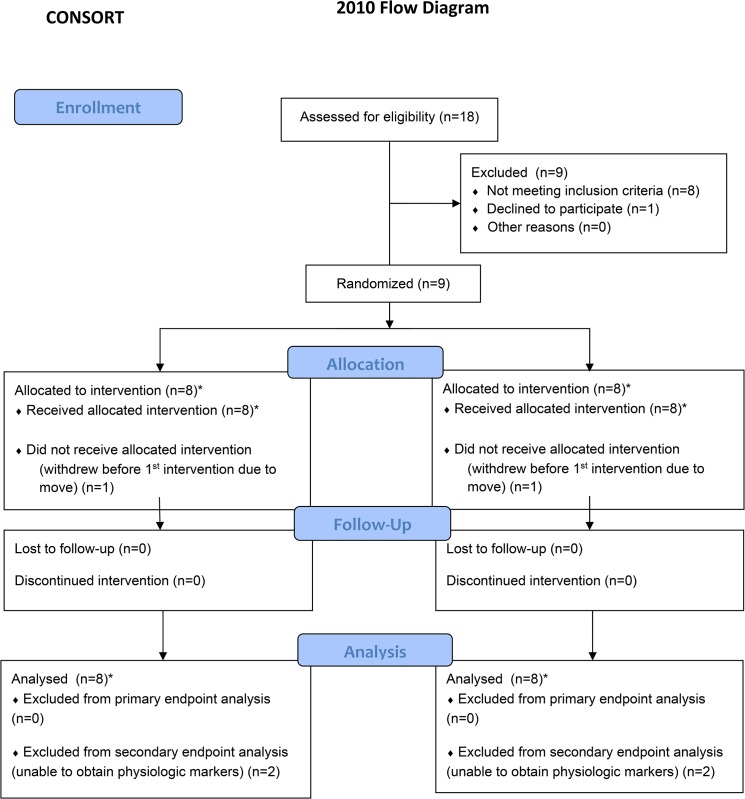
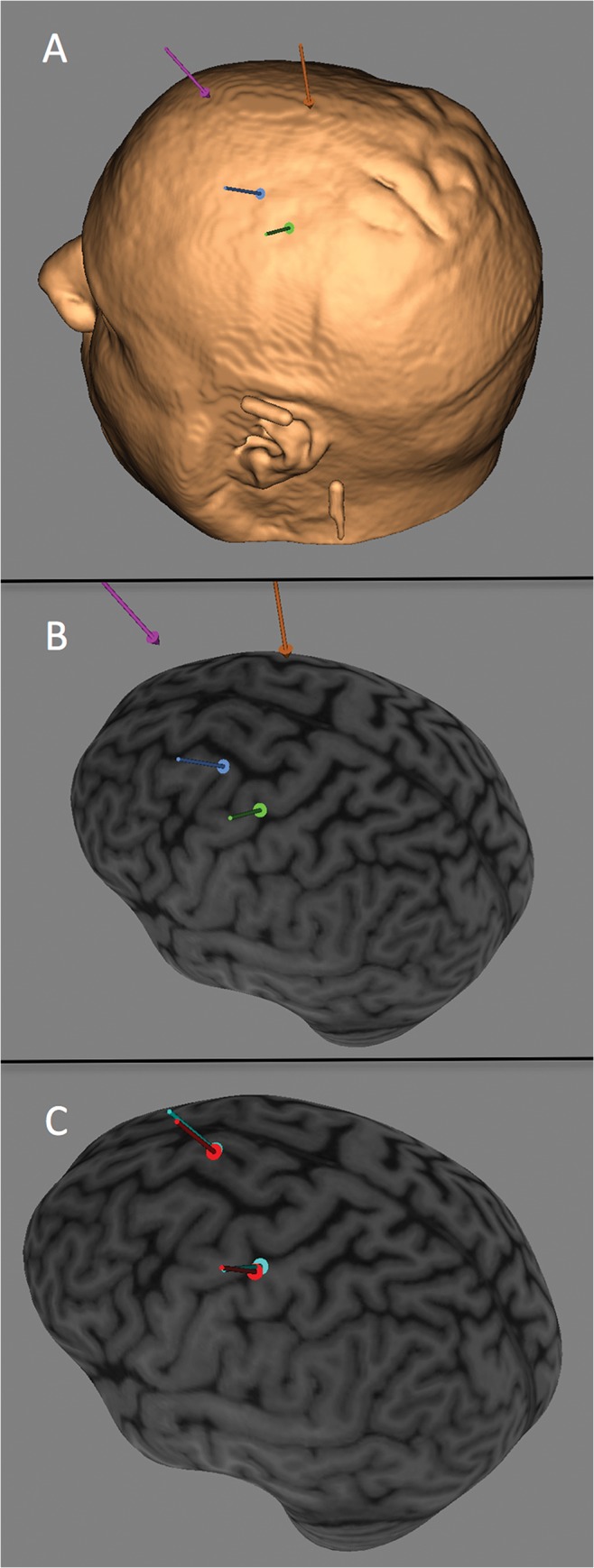
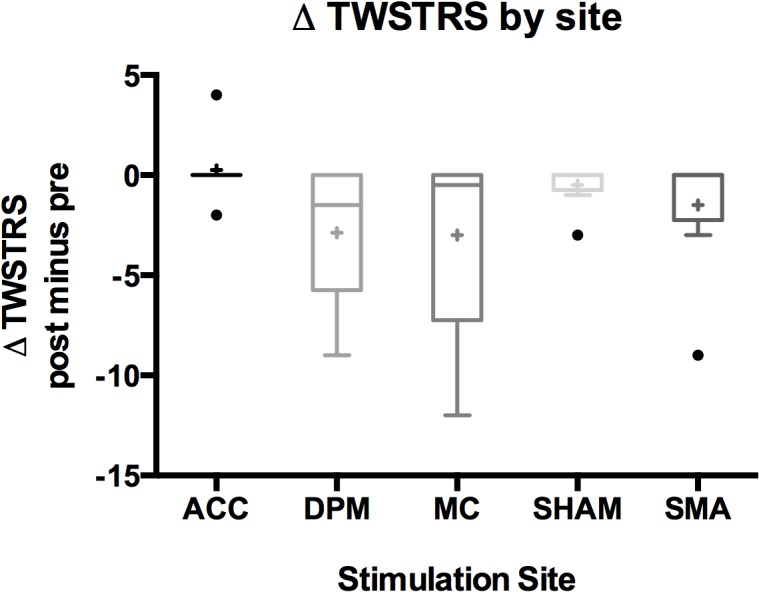
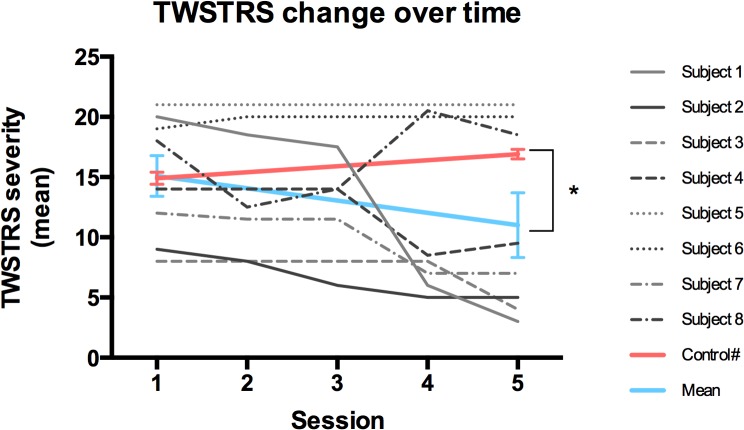
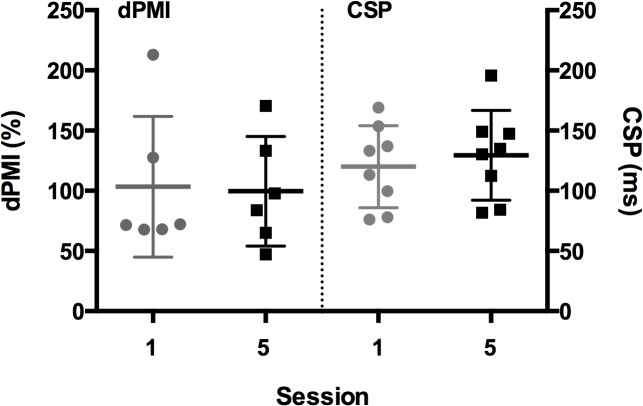
Dystonia is characterized by abnormal posturing due to sustained muscle contraction, which leads to pain and significant disability. New therapeutic targets are needed in this disorder. The objective of this randomized, sham-controlled, blinded exploratory study is to identify a specific motor system target for non-invasive neuromodulation and to evaluate this target in terms of safety and tolerability in the cervical dystonia (CD) population. Eight CD subjects were given 15-minute sessions of low-frequency (0.2 Hz) repetitive transcranial magnetic stimulation (rTMS) over the primary motor cortex (MC), dorsal premotor cortex (dPM), supplementary motor area (SMA), anterior cingulate cortex (ACC) and a sham condition with each session separated by at least two days. The Toronto Western Spasmodic Torticollis Rating Scale (TWSTRS) score was rated in a blinded fashion immediately pre- and post-intervention. Secondary outcomes included physiology and tolerability ratings. The mean change in TWSTRS severity score by site was 0.25 ± 1.7 (ACC), -2.9 ± 3.4 (dPM), -3.0 ± 4.8 (MC), -0.5 ± 1.1 (SHAM), and -1.5 ± 3.2 (SMA) with negative numbers indicating improvement in symptom control. TWSTRS scores decreased from Session 1 (15.1 ± 5.1) to Session 5 (11.0 ± 7.6). The treatment was tolerable and safe. Physiology data were acquired on 6 of 8 subjects and showed no change over time. These results suggest rTMS can modulate CD symptoms. Both dPM and MC are areas to be targeted in further rTMS studies. The improvement in TWSTRS scores over time with multiple rTMS sessions deserves further evaluation.
Trial registration: ClinicalTrials.gov NCT01859247.
Conflict of interest statement
Figures
Similar articles
-
Non-invasive brain stimulation and kinesiotherapy for treatment of focal dystonia: Instrumental analysis of three cases.J Clin Neurosci. 2020 Jun;76:208-210. doi: 10.1016/j.jocn.2020.04.025. Epub 2020 Apr 10. J Clin Neurosci. 2020. PMID: 32284289
-
Motor Cortical Plasticity Relates to Symptom Severity and Clinical Benefit From Deep Brain Stimulation in Cervical Dystonia.Neuromodulation. 2018 Dec;21(8):735-740. doi: 10.1111/ner.12690. Epub 2017 Sep 29. Neuromodulation. 2018. PMID: 28961350
-
A two-site pilot randomized 3 day trial of high dose left prefrontal repetitive transcranial magnetic stimulation (rTMS) for suicidal inpatients.Brain Stimul. 2014 May-Jun;7(3):421-31. doi: 10.1016/j.brs.2014.03.006. Epub 2014 Mar 19. Brain Stimul. 2014. PMID: 24731434 Clinical Trial.
-
A pooled meta-analysis of GPi and STN deep brain stimulation outcomes for cervical dystonia.J Neurol. 2020 May;267(5):1278-1290. doi: 10.1007/s00415-020-09703-9. Epub 2020 Jan 14. J Neurol. 2020. PMID: 31938862
-
Contribution of TMS and rTMS in the Understanding of the Pathophysiology and in the Treatment of Dystonia.Front Neural Circuits. 2016 Nov 10;10:90. doi: 10.3389/fncir.2016.00090. eCollection 2016. Front Neural Circuits. 2016. PMID: 27891079 Free PMC article. Review.
Cited by
-
Transcranial Magnetic Stimulation in Tremor Syndromes: Pathophysiologic Insights and Therapeutic Role.Front Neurol. 2021 Aug 26;12:700026. doi: 10.3389/fneur.2021.700026. eCollection 2021. Front Neurol. 2021. PMID: 34512517 Free PMC article. Review.
-
Research Priorities in Limb and Task-Specific Dystonias.Front Neurol. 2017 May 3;8:170. doi: 10.3389/fneur.2017.00170. eCollection 2017. Front Neurol. 2017. PMID: 28515706 Free PMC article. Review.
-
Abnormal cerebellar processing of the neck proprioceptive information drives dysfunctions in cervical dystonia.Sci Rep. 2018 Feb 2;8(1):2263. doi: 10.1038/s41598-018-20510-1. Sci Rep. 2018. PMID: 29396401 Free PMC article.
-
Applications of Transcranial Magnetic Stimulation for Understanding and Treating Dystonia.Adv Neurobiol. 2023;31:119-139. doi: 10.1007/978-3-031-26220-3_7. Adv Neurobiol. 2023. PMID: 37338699 Review.
-
Treatment of Dystonia: Medications, Neurotoxins, Neuromodulation, and Rehabilitation.Neurotherapeutics. 2020 Oct;17(4):1622-1644. doi: 10.1007/s13311-020-00944-0. Epub 2020 Oct 23. Neurotherapeutics. 2020. PMID: 33095402 Free PMC article. Review.
References
-
- Skogseid IM, Roislien J, Claussen B, Kerty E. Long-term botulinum toxin treatment increases employment rate in patients with cervical dystonia. Mov Disord. 2005;20:1604–1609. - PubMed
-
- Siebner HR, Filipovic SR, Rowe JB, Cordivari C, Gerschlager W, Rothwell JC, et al. Patients with focal arm dystonia have increased sensitivity to slow-frequency repetitive TMS of the dorsal premotor cortex. Brain. 2003;126;2710–2725. - PubMed
-
- Murase N, Rothwell JC, Kaji R, Urushihara R, Nakamura K, Murayama N, et al. Subthreshold low-frequency repetitive transcranial magnetic stimulation over the premotor cortex modulates writer’s cramp. Brain. 2005;128:104–115. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
