

Giant solitary fibrous tumor of the pelvis successfully treated with preoperative embolization and surgical resection: a case report
- PMID: 25924672
- PMCID: PMC4417519
- DOI: 10.1186/s12957-015-0578-6
Giant solitary fibrous tumor of the pelvis successfully treated with preoperative embolization and surgical resection: a case report
Abstract
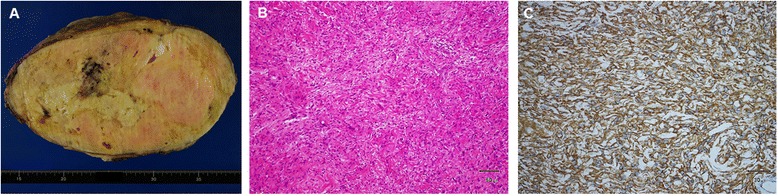
Solitary fibrous tumors (SFTs) rarely develop in the pelvis. When they do arise, they are usually treated using surgery, although SFTs are often very large by the time of diagnosis, which makes surgical excision difficult. We report a case of a 63-year-old man who was referred to our hospital for the treatment of a giant tumor of the pelvis. Computed tomography (CT) revealed a 30 × 25 × 19 cm sized hypervascular tumor that almost completely filled the pelvic cavity. The diagnosis of SFT was made by CT-assisted needle biopsy. The feeding arteries of the tumor were embolized twice. The first embolization aimed to reduce the tumor volume, while the second one was planned a day prior to the surgery to obtain hematostasis during the operation. Tumor resection was then performed. The blood loss during the operation was 440 ml, and there was no uncontrollable bleeding. The postoperative course was uneventful. No recurrence of SFT was observed during a 2-year follow-up.
Figures

Similar articles
-
Solitary fibrous tumor in the abdomen and pelvis: A case series with radiological findings and treatment recommendations.Clin Imaging. 2018 Mar-Apr;48:48-54. doi: 10.1016/j.clinimag.2017.10.002. Epub 2017 Oct 7. Clin Imaging. 2018. PMID: 29028514
-
Trans-sacral resection of a solitary fibrous tumor in the pelvis: report of a case.Surg Today. 2011 Nov;41(11):1548-51. doi: 10.1007/s00595-010-4535-2. Epub 2011 Oct 4. Surg Today. 2011. PMID: 21969160 Review.
-
Solitary fibrous tumor of the pelvis treated with preoperative embolization and pelvic exenteration.Am Surg. 2011 Jan;77(1):112-3. Am Surg. 2011. PMID: 21396319 No abstract available.
-
A giant solitary fibrous tumor of the abdominal pelvic cavity: A case report and literature review.Medicine (Baltimore). 2024 Aug 9;103(32):e39270. doi: 10.1097/MD.0000000000039270. Medicine (Baltimore). 2024. PMID: 39121255 Free PMC article. Review.
-
[Solitary fibrous tumor in the pelvic space: a case report].Hinyokika Kiyo. 2007 Dec;53(12):897-901. Hinyokika Kiyo. 2007. PMID: 18203530 Japanese.
Cited by
-
A Rare Case of a Pelvic Solitary Fibrous Tumor.Cureus. 2022 Mar 31;14(3):e23686. doi: 10.7759/cureus.23686. eCollection 2022 Mar. Cureus. 2022. PMID: 35505761 Free PMC article.
-
Radiological findings in pelvic solitary fibrous tumour.BJR Case Rep. 2016 Nov 2;2(4):20150373. doi: 10.1259/bjrcr.20150373. eCollection 2016. BJR Case Rep. 2016. PMID: 30460023 Free PMC article.
-
A solitary fibrous tumour mimicking an aggressive angiomyxoma/liposarcoma.BMJ Case Rep. 2017 May 5;2017:bcr2016218202. doi: 10.1136/bcr-2016-218202. BMJ Case Rep. 2017. PMID: 28476856 Free PMC article.
-
Postoperative Morbidity After Radical Resection of Retroperitoneal Solitary Fibrous Tumor.Front Surg. 2022 Mar 28;9:833296. doi: 10.3389/fsurg.2022.833296. eCollection 2022. Front Surg. 2022. PMID: 35419405 Free PMC article.
-
A rare solitary fibrous tumor in the ischiorectal fossa: a case report.Surg Case Rep. 2018 Oct 3;4(1):126. doi: 10.1186/s40792-018-0533-1. Surg Case Rep. 2018. PMID: 30284069 Free PMC article.
References
-
- Klemperer P, Rabin CB. Primary neoplasms of the pleura: a report of five cases. Arch Pathol. 1931;11:385–412.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
