

Development and validation of a scalable next-generation sequencing system for assessing relevant somatic variants in solid tumors
- PMID: 25925381
- PMCID: PMC4415141
- DOI: 10.1016/j.neo.2015.03.004
Development and validation of a scalable next-generation sequencing system for assessing relevant somatic variants in solid tumors
Abstract
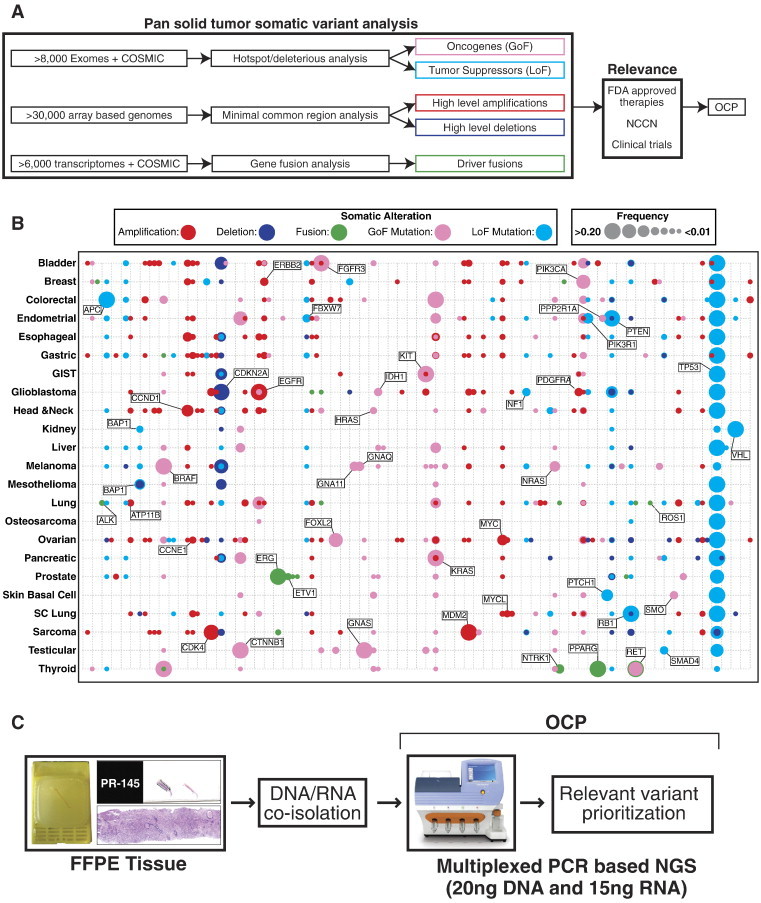
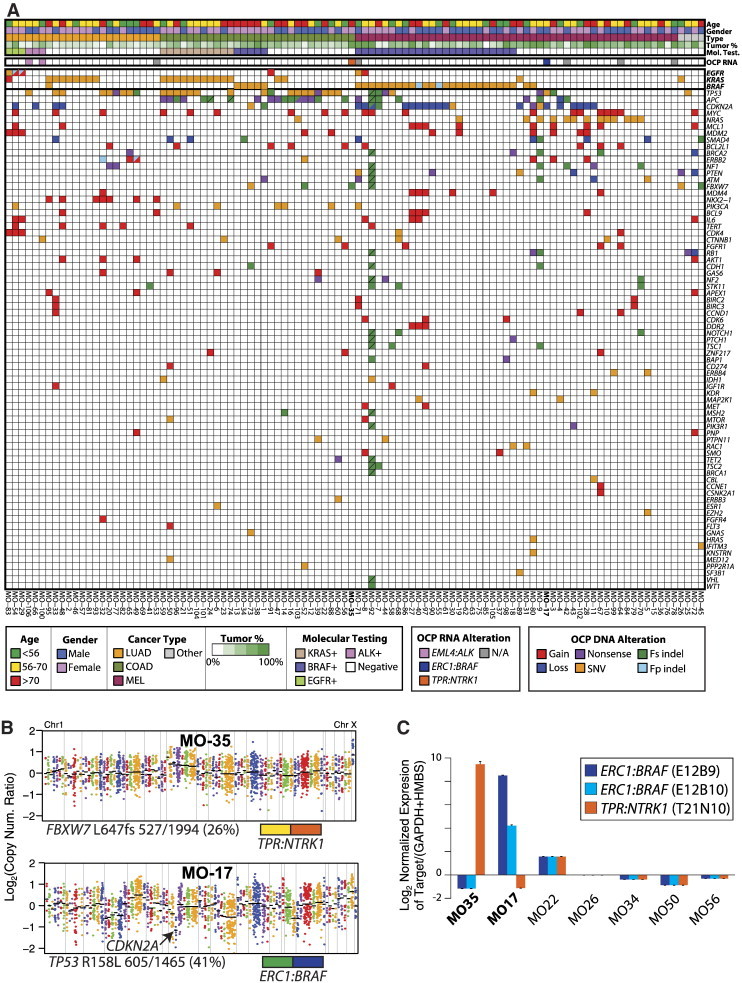
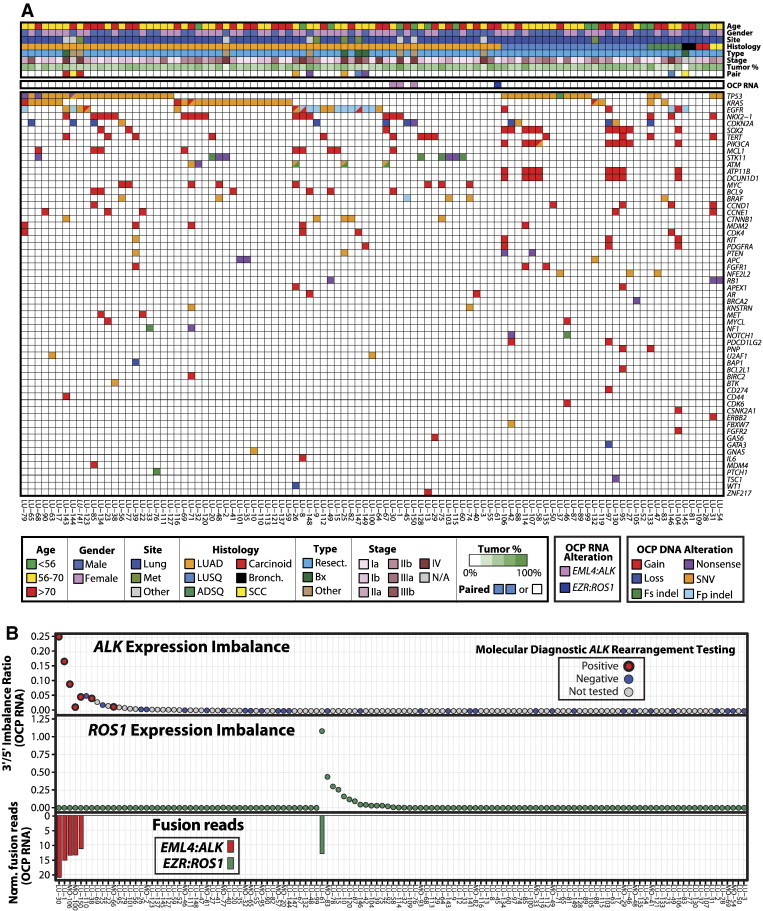
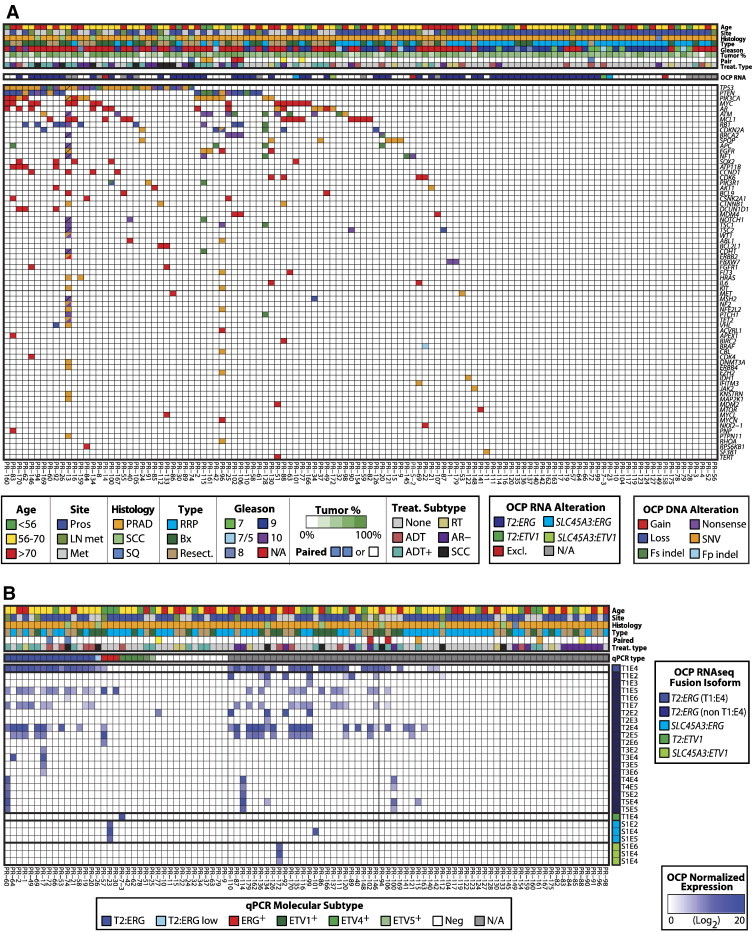
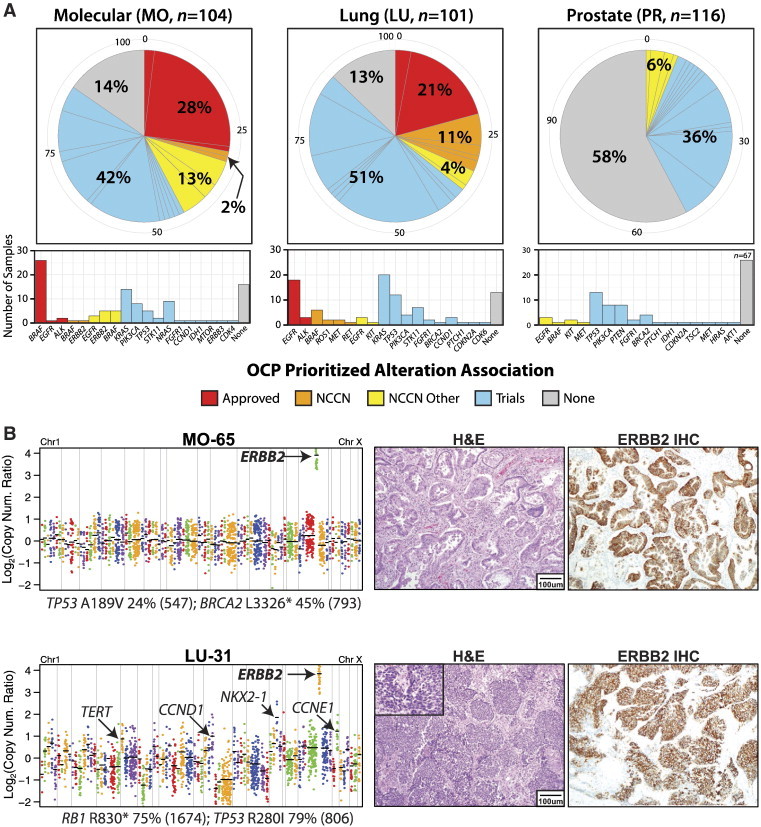
Next-generation sequencing (NGS) has enabled genome-wide personalized oncology efforts at centers and companies with the specialty expertise and infrastructure required to identify and prioritize actionable variants. Such approaches are not scalable, preventing widespread adoption. Likewise, most targeted NGS approaches fail to assess key relevant genomic alteration classes. To address these challenges, we predefined the catalog of relevant solid tumor somatic genome variants (gain-of-function or loss-of-function mutations, high-level copy number alterations, and gene fusions) through comprehensive bioinformatics analysis of >700,000 samples. To detect these variants, we developed the Oncomine Comprehensive Panel (OCP), an integrative NGS-based assay [compatible with <20 ng of DNA/RNA from formalin-fixed paraffin-embedded (FFPE) tissues], coupled with an informatics pipeline to specifically identify relevant predefined variants and created a knowledge base of related potential treatments, current practice guidelines, and open clinical trials. We validated OCP using molecular standards and more than 300 FFPE tumor samples, achieving >95% accuracy for KRAS, epidermal growth factor receptor, and BRAF mutation detection as well as for ALK and TMPRSS2:ERG gene fusions. Associating positive variants with potential targeted treatments demonstrated that 6% to 42% of profiled samples (depending on cancer type) harbored alterations beyond routine molecular testing that were associated with approved or guideline-referenced therapies. As a translational research tool, OCP identified adaptive CTNNB1 amplifications/mutations in treated prostate cancers. Through predefining somatic variants in solid tumors and compiling associated potential treatment strategies, OCP represents a simplified, broadly applicable targeted NGS system with the potential to advance precision oncology efforts.
Copyright © 2015 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Garraway LA, Verweij J, Ballman KV. Precision oncology: an overview. J Clin Oncol. 2013;31:1803–1805. - PubMed
-
- Mendelsohn J. Personalizing oncology: perspectives and prospects. J Clin Oncol. 2013;31:1904–1911. - PubMed
-
- Arteaga CL, Baselga J. Impact of genomics on personalized cancer medicine. Clin Cancer Res. 2012;18:612–618. - PubMed
-
- McDermott U, Downing JR, Stratton MR. Genomics and the continuum of cancer care. N Engl J Med. 2011;364:340–350. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
