

Effect of preoperative neuromuscular training (NEMEX-TJR) on functional outcome after total knee replacement: an assessor-blinded randomized controlled trial
- PMID: 25925404
- PMCID: PMC4414282
- DOI: 10.1186/s12891-015-0556-8
Effect of preoperative neuromuscular training (NEMEX-TJR) on functional outcome after total knee replacement: an assessor-blinded randomized controlled trial
Abstract
Background: Improving functional status preoperatively through exercise may improve postoperative outcome. Previous knowledge on preoperative exercise in knee osteoarthritis is insufficient. The aim of the study was to compare the difference in change between groups in lower extremity function from baseline to 3 months after Total Knee Replacement (TKR) following a neuromuscular exercise programme (NEMEX-TJR) plus a knee school educational package (KS) or KS alone.
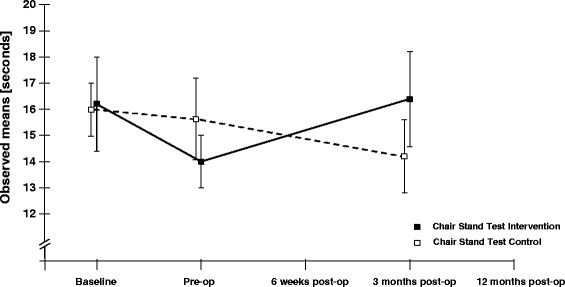
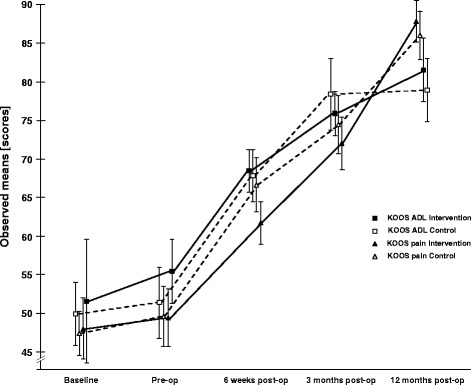
Methods: 45 patients (55-83 years, 53% male, waiting for TKR) were randomized to receive a minimum of 8 sessions of NEMEXTJR plus 3 sessions of KS or 3 sessions of KS alone. Function was assessed with the Chair Stand Test (CST, primary endpoint) and the Knee Injury and Osteoarthritis Outcome Score (KOOS) subscales focusing on daily living function (ADL) and pain (secondary endpoints). Assessments were performed immediately before and after the intervention, and at 6 weeks, 3 months and 12 months after surgery by a physiotherapist, blinded to group allocation.
Results: After intervention before surgery we observed a small improvement for primary and secondary endpoints in both groups, which did not differ significantly between groups: comparing the exercise to the control group the treatment effect for the CST was -1.5 seconds (95% CI: -5.3, 2.2), for KOOS ADL and KOOS pain the treatment effect was 1.3 points (-10.1, 12.8) and -2.3 (-12.4, 7.9) respectively. At 3 months after surgery we observed a small improvement in the primary endpoint in the control group and a significant improvement in the secondary endpoints in both exercise and control groups, which did not differ significantly between groups: comparing the exercise group to the control group the treatment effect in the CST was 2.0 seconds (-1.8, 5.8), for KOOS ADL and KOOS pain the treatment effect was -4.9 points (-16.3, 6.5) and -3.3 points (-13.5, 6.8) respectively.
Conclusions: A median (IQR) of 10 (8, 14) exercise sessions before surgery showed an additional small but non-significant improvement in all functional assessments compared to patient education alone. These benefits were not sustained after TKR. Our trial doesn't give a conclusive answer to whether additional preoperative exercise on postoperative functional outcomes is beneficial.
Figures

References
-
- Seed SM, Dunican KC, Lynch AM. Osteoarthritis: a review of treatment options. Geriatrics. 2009;64(10):20–9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
