

The hyper-reactive malarial splenomegaly: a systematic review of the literature
- PMID: 25925423
- PMCID: PMC4438638
- DOI: 10.1186/s12936-015-0694-3
The hyper-reactive malarial splenomegaly: a systematic review of the literature
Abstract
Background: The hyper-reactive malarial splenomegaly syndrome (HMS) is a leading cause of massive splenomegaly in malaria-endemic countries. HMS is caused by a chronic antigenic stimulation derived from the malaria parasite. Classic Fakunle's major criteria for case definition are: persistent gross splenomegaly, elevated anti-malarial antibodies, IgM titre >2 SD above the local mean value and favourable response to long-term malaria prophylaxis. The syndrome is fatal if left untreated. The aim of this study is to systematically review the literature about HMS, particularly focussing on case definition, epidemiology and management.
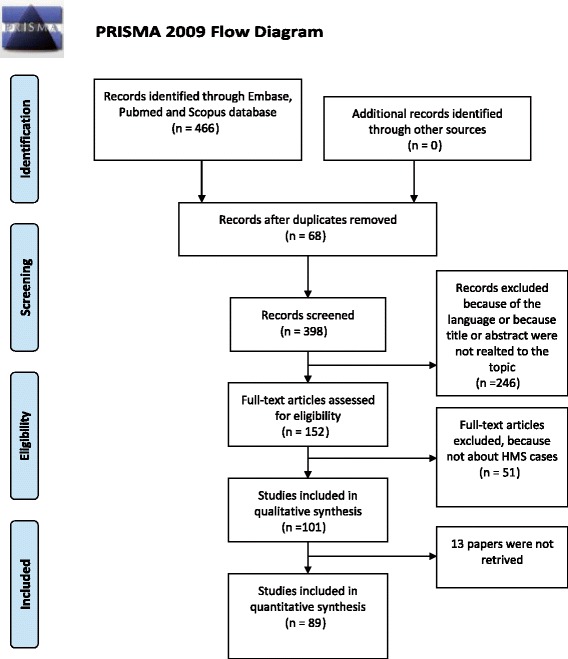
Methods: The search strategy was based on the following database sources: Pubmed, EmBase, Scopus. Search was done in March, 2014 and limited to English, Spanish, Italian, French, and Portuguese.
Results: Papers detected were 149, of which 89 were included. Splenomegaly was variably defined and the criterion of increased IgM was not always respected. The highest prevalence was reported in Papua New Guinea (up to 80%). In different African countries, 31 to 76% of all splenomegalies were caused by HMS. Fatality rate reached 36% in three years. The most frequent anti-malarial treatments administered were weekly chloroquine or daily proguanil from a minimum of one month to lifelong. In non-endemic countries, a few authors opted for a single, short anti-malarial treatment. All treated patients with no further exposure improved. Cases not completely fulfilling Fakunle's criteria and therefore untreated, subsequently evolved into HMS. It seems thus appropriate to treat incomplete or 'early' HMS, too.
Conclusions: For patients not re-exposed to endemic areas, a short course of treatment is sufficient, showing that eradicating the infection is sufficient to cure HMS. Longer (probably lifelong) courses, or intermittent treatments, are required for those who remain exposed. Splenectomy, associated with high mortality, should be strictly limited to cases not responding to medical treatment.
Figures

References
-
- Crane G. Recent studies of hyperreactive malarious splenomegaly (tropical splenomegaly syndrome) in Papua New Guinea. P N G Med J. 1986;29:35–40. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
