

An automatically contamination-avoiding technique for intracorporeal esophagojejunostomy using a transorally inserted anvil during laparoscopic total gastrectomy for gastric cancer
- PMID: 25926082
- PMCID: PMC4411702
- DOI: 10.1186/s12957-015-0563-0
An automatically contamination-avoiding technique for intracorporeal esophagojejunostomy using a transorally inserted anvil during laparoscopic total gastrectomy for gastric cancer
Abstract
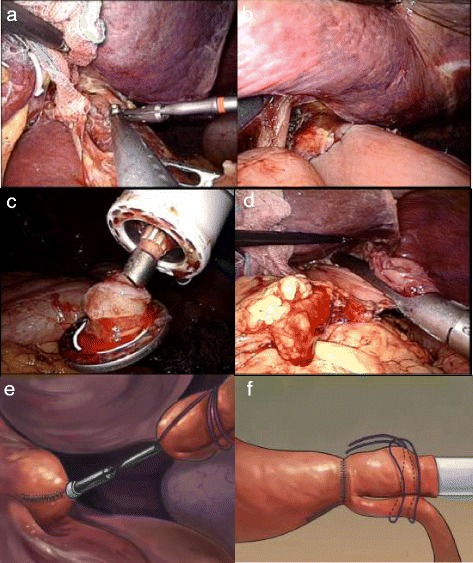
Background: Intracorporeal Roux-en-Y esophagojejunostomy during laparoscopic total gastrectomy for gastric cancer remains a challenging manipulation due to the uncontrolled direction of the jejunal side or unintended embedded tissues, although several methods have been introduced. In this study, we simplified the procedure based on a surgical string fixing technique using a transorally inserted anvil (OrVil™; Covidien Ltd., Mansfield, MA, USA).
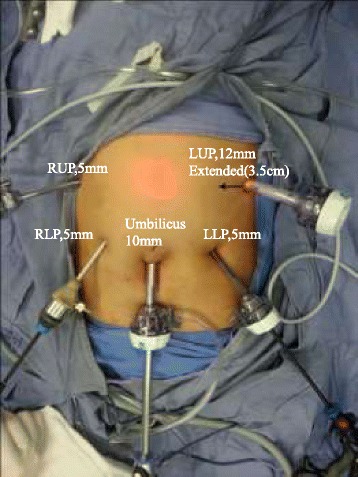
Methods: From March 2012 to September 2013, 14 consecutive patients underwent simplified intracorporeal Roux-en-Y esophagojejunostomy using OrVil™ during laparoscopic total gastrectomy for gastric cancer at our hospital. Clinicopathologic characteristics and surgical outcomes of these patients were retrospectively analyzed.
Results: All of the procedures were successful completed with no complication or conversion to open surgery. The mean overall operative time was 193.8 ± 41.8 min, whereas the mean reconstruction time was 32.6 ± 4.6 min. The mean estimated blood loss was 105.7 ± 65.4 ml. The mean diameter of anastomosis measured by upper gastrointestinal contrast X-ray test at 1 month after operation was 2.3 cm. During a median follow-up period of 12 months, neither local recurrence nor anastomosis-related morbidity was observed.
Conclusions: Our preliminary results suggested that this automatically contamination-avoiding technique based on a surgical-string-fixing strategy using OrVil™ during laparoscopic total gastrectomy for gastric cancer might be feasible and safe and provide a simple solution for intracorporeal Roux-en-Y esophagojejunostomy.
Figures



References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
