

Global access to surgical care: a modelling study
- PMID: 25926087
- PMCID: PMC4820251
- DOI: 10.1016/S2214-109X(15)70115-4
Global access to surgical care: a modelling study
Abstract
Background: More than 2 billion people are unable to receive surgical care based on operating theatre density alone. The vision of the Lancet Commission on Global Surgery is universal access to safe, affordable surgical and anaesthesia care when needed. We aimed to estimate the number of individuals worldwide without access to surgical services as defined by the Commission's vision.
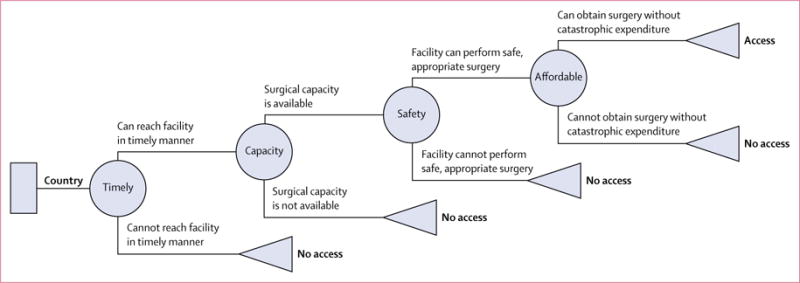
Methods: We modelled access to surgical services in 196 countries with respect to four dimensions: timeliness, surgical capacity, safety, and affordability. We built a chance tree for each country to model the probability of surgical access with respect to each dimension, and from this we constructed a statistical model to estimate the proportion of the population in each country that does not have access to surgical services. We accounted for uncertainty with one-way sensitivity analyses, multiple imputation for missing data, and probabilistic sensitivity analysis.
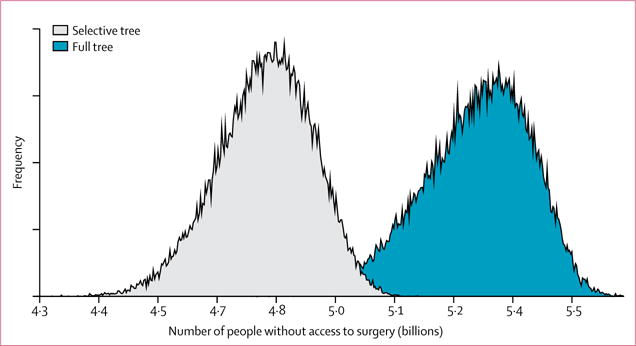
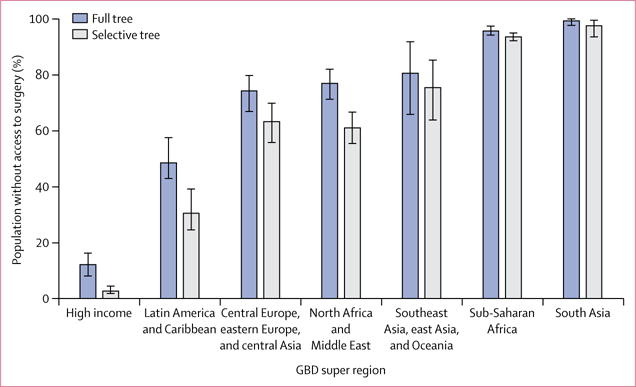
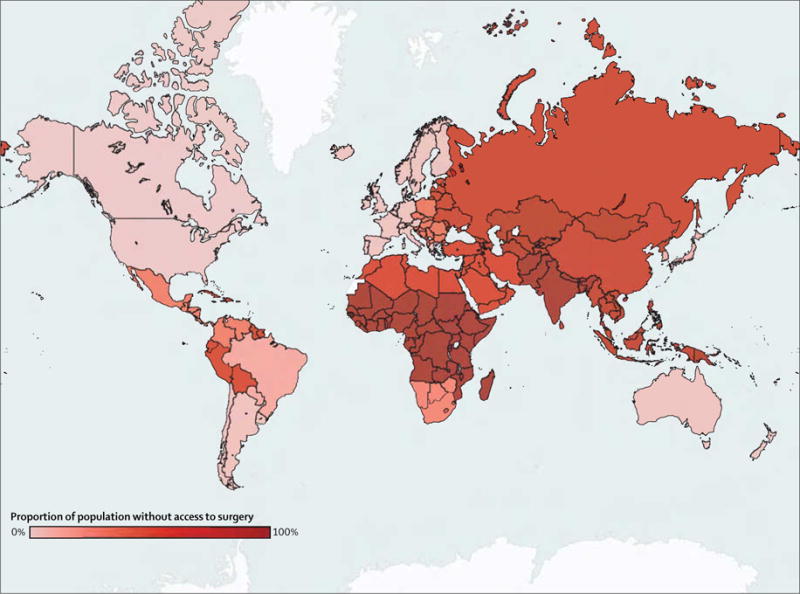
Findings: At least 4·8 billion people (95% posterior credible interval 4·6-5·0 [67%, 64-70]) of the world's population do not have access to surgery. The proportion of the population without access varied widely when stratified by epidemiological region: greater than 95% of the population in south Asia and central, eastern, and western sub-Saharan Africa do not have access to care, whereas less than 5% of the population in Australasia, high-income North America, and western Europe lack access.
Interpretation: Most of the world's population does not have access to surgical care, and access is inequitably distributed. The near absence of access in many low-income and middle-income countries represents a crisis, and as the global health community continues to support the advancement of universal health coverage, increasing access to surgical services will play a central role in ensuring health care for all.
Funding: None.
Copyright © 2015 Alkire et al. Open Access article distributed under the terms of CC BY. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
We declare no competing interests.
Figures
Comment in
-
The surgery spring.Lancet Glob Health. 2015 Jun;3(6):e297. doi: 10.1016/S2214-109X(15)00015-7. Epub 2015 May 12. Lancet Glob Health. 2015. PMID: 25979513 No abstract available.
-
Global access to surgical care: moving forward.Lancet Glob Health. 2015 Jun;3(6):e298-9. doi: 10.1016/S2214-109X(15)00004-2. Lancet Glob Health. 2015. PMID: 26001569 No abstract available.
-
Strengthening health systems through surgery.Lancet. 2024 Jun 1;403(10442):2358-2360. doi: 10.1016/S0140-6736(24)01031-6. Epub 2024 May 20. Lancet. 2024. PMID: 38782001 No abstract available.
References
-
- Meara JG, Leather AJM, Hagander L, et al. Global surgery 2030: evidence and solutions for achieving health, welfare, and economic development. Lancet. 2015 published online April 27. http://dx.doi.org/10.1016/S0140-6736(15)60160-X. - DOI - PubMed
-
- Kim JY, Farmer PE. What’s missing from the Ebola fight in West Africa. The Washington Post. 2014 Aug 31, 2014.
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. Lancet. 2008;372:139–44. - PubMed
-
- Funk LM, Weiser TG, Berry WR, et al. Global operating theatre distribution and pulse oximetry supply: an estimation from reported data. Lancet. 2010;376:1055–61. - PubMed
-
- Banerjee JK. Analysing outcome of surgical development–rural surgery as an example. Indian J Surg. 2003;65:68–72.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
