

The Volume-Outcome Relationship in Critical Care: A Systematic Review and Meta-analysis
- PMID: 25927593
- PMCID: PMC4493880
- DOI: 10.1378/chest.14-2195
The Volume-Outcome Relationship in Critical Care: A Systematic Review and Meta-analysis
Abstract
Objective: The purpose of this study was to systematically review the research on volume and outcome relationships in critical care.
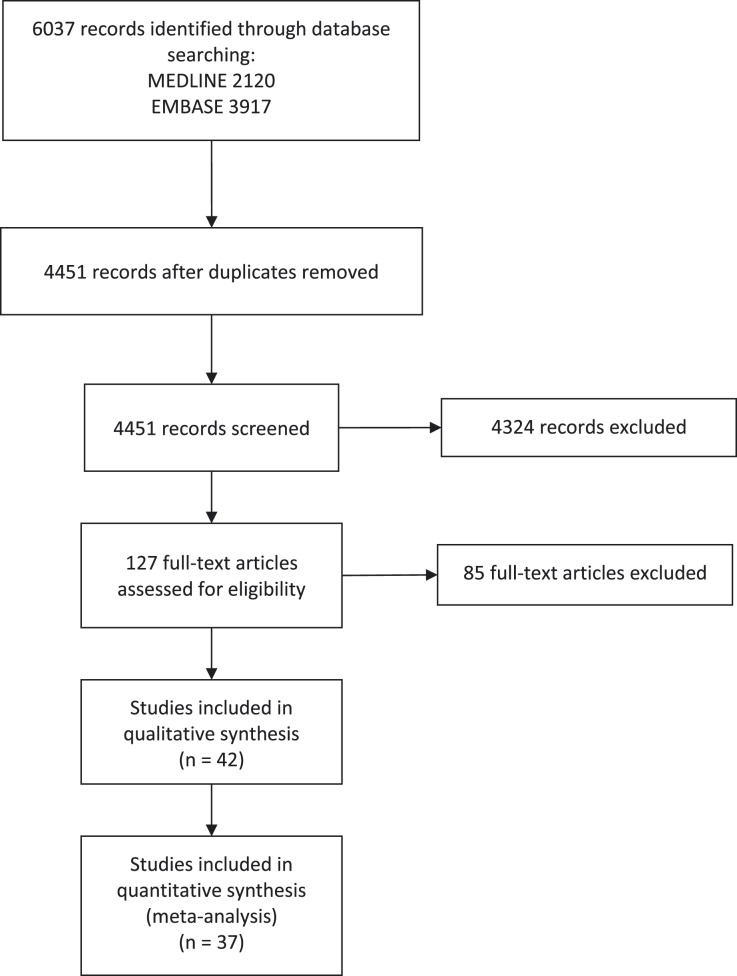
Methods: From January 1, 2001, to April 30, 2014, MEDLINE and EMBASE were searched for studies assessing the relationship between admission volume and clinical outcomes in critical illness. Bibliographies were reviewed to identify other articles of interest, and experts were contacted about missing or unpublished studies. Of 127 studies reviewed, 46 met inclusion criteria, covering seven clinical conditions. Two investigators independently reviewed each article using a standardized form to abstract information on key study characteristics and results.
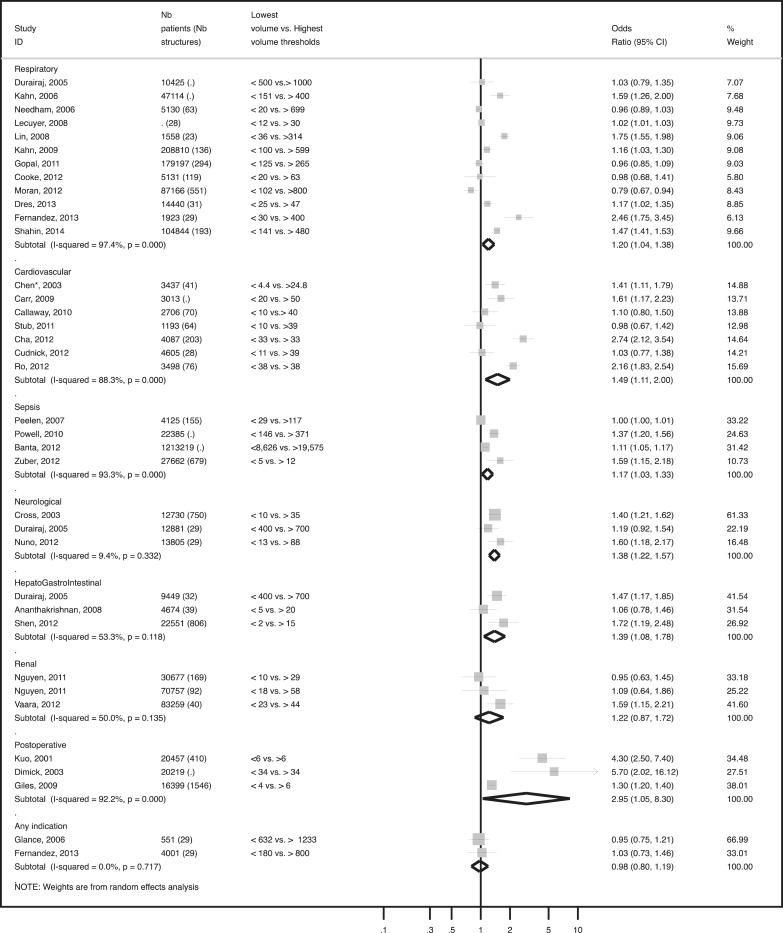
Results: Overall, 29 of the studies (63%) reported a statistically significant association between higher admission volume and improved outcomes. The magnitude of the association (mortality OR between the lowest vs highest stratum of volume centers), as well as the thresholds used to characterize high volume, varied across clinical conditions. Critically ill patients with cardiovascular (n = 7, OR = 1.49 [1.11-2.00]), respiratory (n = 12, OR = 1.20 [1.04-1.38]), severe sepsis (n = 4, OR = 1.17 [1.03-1.33]), hepato-GI (n = 3, OR = 1.30 [1.08-1.78]), neurologic (n = 3, OR = 1.38 [1.22-1.57]), and postoperative admission diagnoses (n = 3, OR = 2.95 [1.05-8.30]) were more likely to benefit from admission to higher-volume centers compared with lower-volume centers. Studies that controlled for ICU or hospital organizational factors were less likely to find a significant volume-outcome relationship than studies that did not control for these factors.
Conclusions: Critically ill patients generally benefit from care in high-volume centers, with more substantial benefits in selected high-risk conditions. This relationship may in part be mediated by specific ICU and hospital organizational factors.
Figures

References
-
- Halm EA, Lee C, Chassin MR. Is volume related to outcome in health care? A systematic review and methodologic critique of the literature. Ann Intern Med. 2002;137(6):511-520. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346(15):1128-1137. - PubMed
-
- Kanhere MH, Kanhere HA, Cameron A, Maddern GJ. Does patient volume affect clinical outcomes in adult intensive care units? Intensive Care Med. 2012;38(5):741-751. - PubMed
-
- Nguyen YL, Kahn JM, Angus DC. Reorganizing adult critical care delivery: the role of regionalization, telemedicine, and community outreach. Am J Respir Crit Care Med. 2010;181(11):1164-1169. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
