

Effect of initial calorie intake via enteral nutrition in critical illness: a meta-analysis of randomised controlled trials
- PMID: 25927829
- PMCID: PMC4434568
- DOI: 10.1186/s13054-015-0902-0
Effect of initial calorie intake via enteral nutrition in critical illness: a meta-analysis of randomised controlled trials
Abstract
Introduction: Guidelines support the use of enteral nutrition to improve clinical outcomes in critical illness; however, the optimal calorie and protein intake remains unclear. The purpose of this meta-analysis was to quantitatively analyze randomised controlled trials with regard to clinical outcomes related to varying calorie and protein administration in critically ill adult patients.
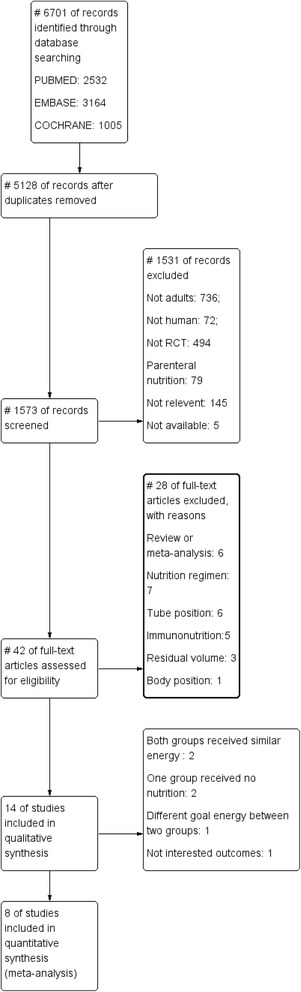
Method: We searched Medline, EMBASE, and Cochrane databases to identify randomised controlled trials that compared the effects of initially different calorie and protein intake in critical illness. The risk ratio (RR) and weighted mean difference with 95% confidence intervals (CI) were calculated using random-effects models. The primary endpoint was mortality; secondary endpoints included infection, pneumonia, gastrointestinal intolerance, hospital and intensive care unit lengths of stay, and mechanical ventilation days.
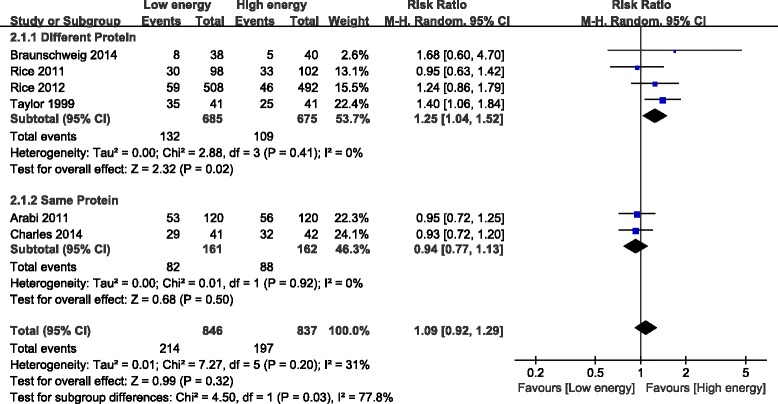
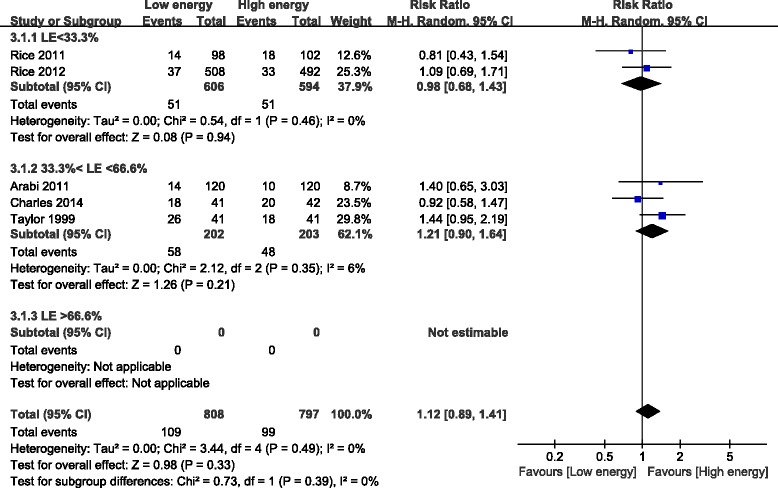
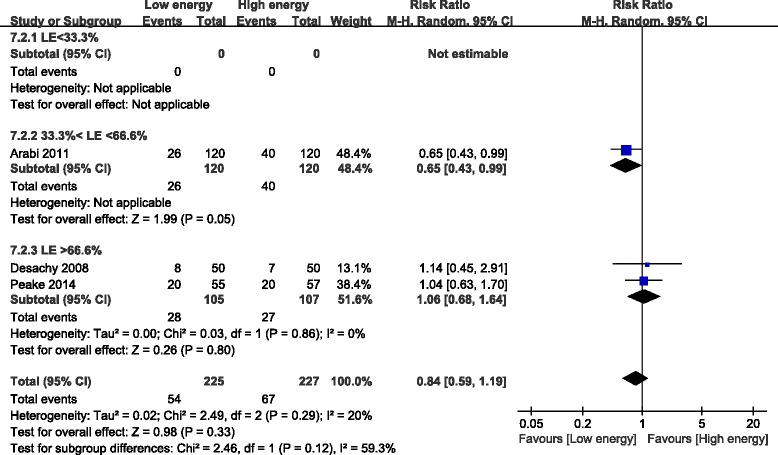
Results: In the eight randomised controlled trials that enrolled 1,895 patients there was no statistical difference between the low-energy and high-energy groups in mortality (RR, 0.90; 95% CI, 0.71 to 1.15; P = 0.40), infection (RR, 1.09; 95% CI, 0.92 to 1.29; P = 0.32), or the risk of gastrointestinal intolerance (RR, 0.84; 95% CI, 0.59 to 1.19; P = 0.33). In subgroup analysis, the low-energy subgroup, fed 33.3 to 66.6% of goal energy, showed a lower mortality than the high-energy group (RR, 0.68; 95% CI, 0.51 to 0.92; P = 0.01). The improvements in mortality and gastrointestinal intolerance were absent when calorie intake was >66.6% of goal energy in the low-energy group. High-energy intake combined with high-protein intake reduced the infections (RR, 1.25; 95% CI, 1.04 to 1.52; P = 0.02); however, when the daily protein intake was similar in both groups, a high-energy intake did not decrease the infections. No statistical differences were observed in other secondary outcomes.
Conclusion: This meta-analysis indicates that high-energy intake does not improve outcomes and may increase complications in critically ill patients who are not malnourished. Initial moderate nutrient intake (33.3 to 66.6% of goal energy), compared to high energy, may reduce mortality, and a higher protein intake combined with high energy (≥ 0.85 g/kg per day) may decrease the infection rate. However, the contribution of energy versus protein intake to outcomes remains unknown.
Figures





References
-
- Alverdy JC, Aoys E, Moss GS. Total parenteral nutrition promotes bacterial translocation from the gut. Surgery. 1988;104:185–90. - PubMed
-
- Martindale RG, McClave SA, Vanek VW, McCarthy M, Roberts P, Taylor B, et al. Guidelines for the provision and assessment of nutrition support therapy in the adult critically ill patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition: Executive Summary. Crit Care Med. 2009;37:1757–61. doi: 10.1097/CCM.0b013e3181a40116. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
