

Heterogeneity of synovial molecular patterns in patients with arthritis
- PMID: 25927832
- PMCID: PMC4415786
- DOI: 10.1371/journal.pone.0122104
Heterogeneity of synovial molecular patterns in patients with arthritis
Abstract
Objectives: Early diagnosis of rheumatoid arthritis (RA) is an unmet medical need in the field of rheumatology. Previously, we performed high-density transcriptomic studies on synovial biopsies from patients with arthritis, and found that synovial gene expression profiles were significantly different according to the underlying disorder. Here, we wanted to further explore the consistency of the gene expression signals in synovial biopsies of patients with arthritis, using low-density platforms.
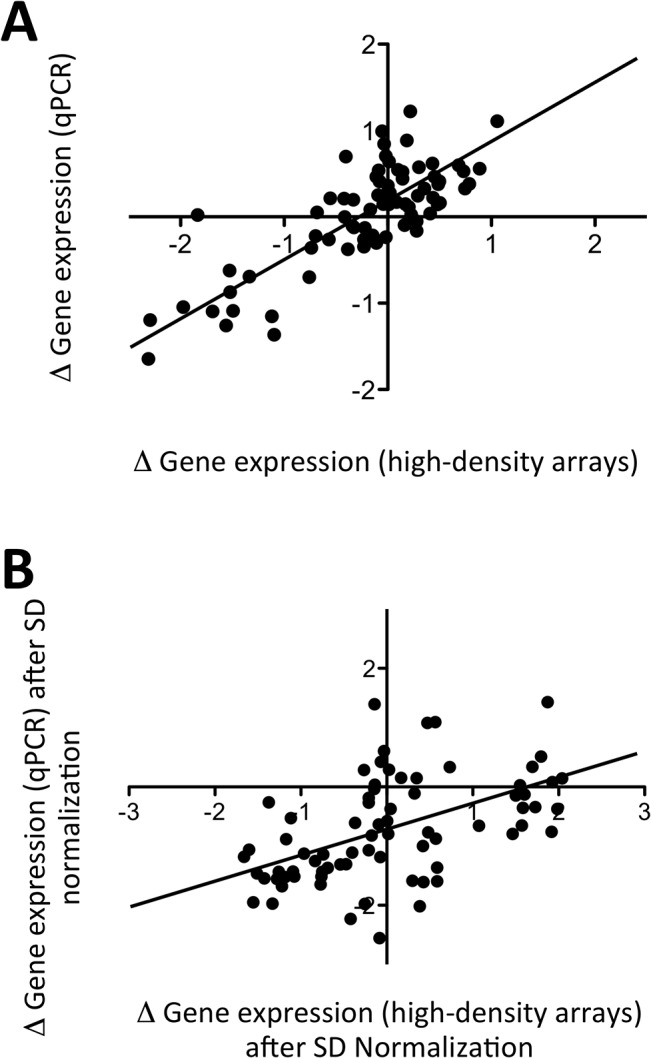
Methods: Low-density assays (cDNA microarray and microfluidics qPCR) were designed, based on the results of the high-density microarray data. Knee synovial biopsies were obtained from patients with RA, spondyloarthropathies (SA) or osteoarthritis (OA) (n = 39), and also from patients with initial undifferentiated arthritis (UA) (n = 49).
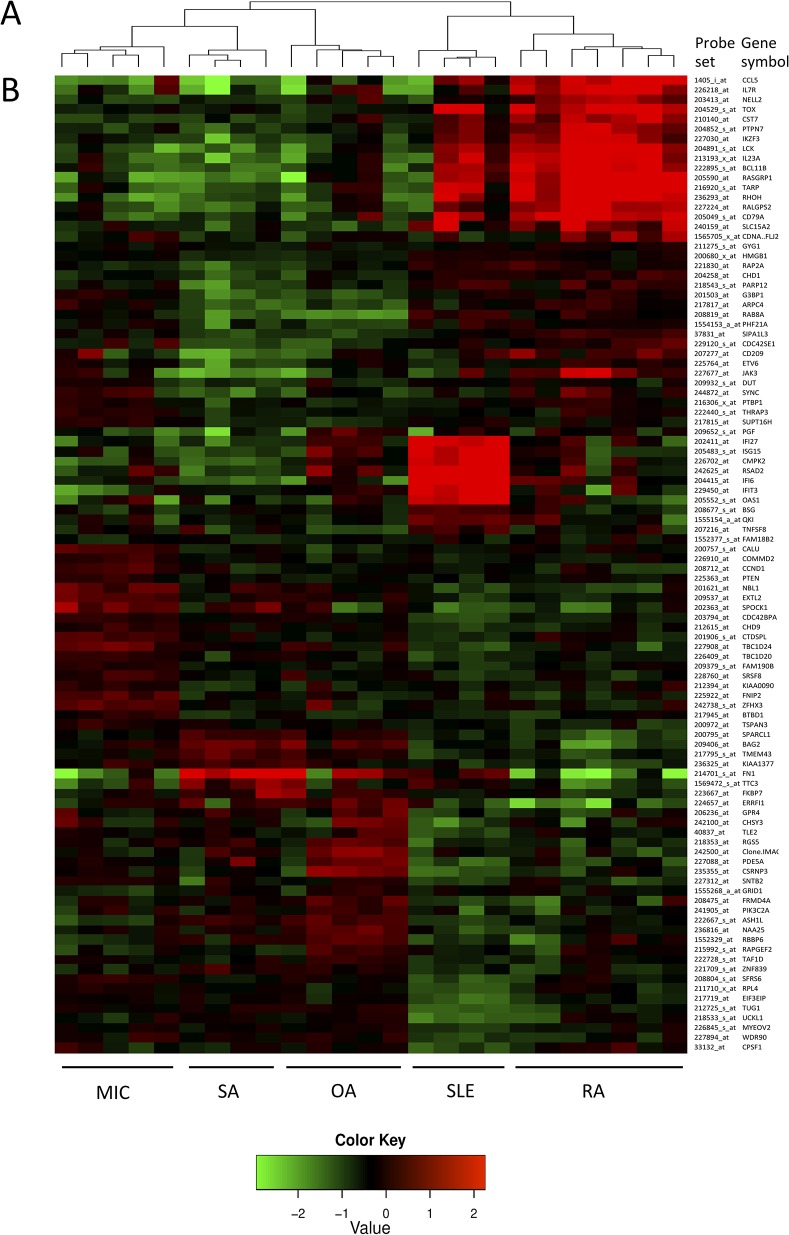
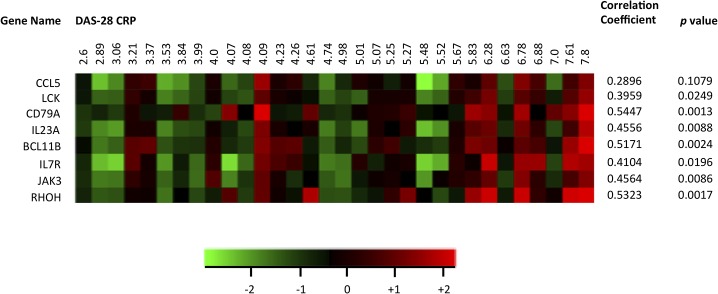
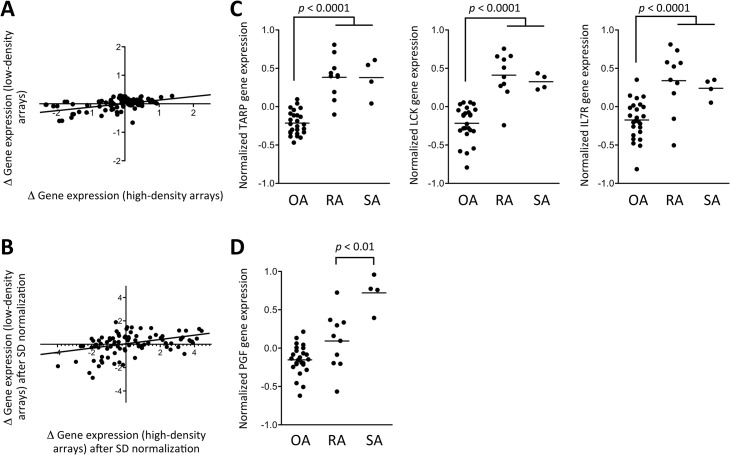
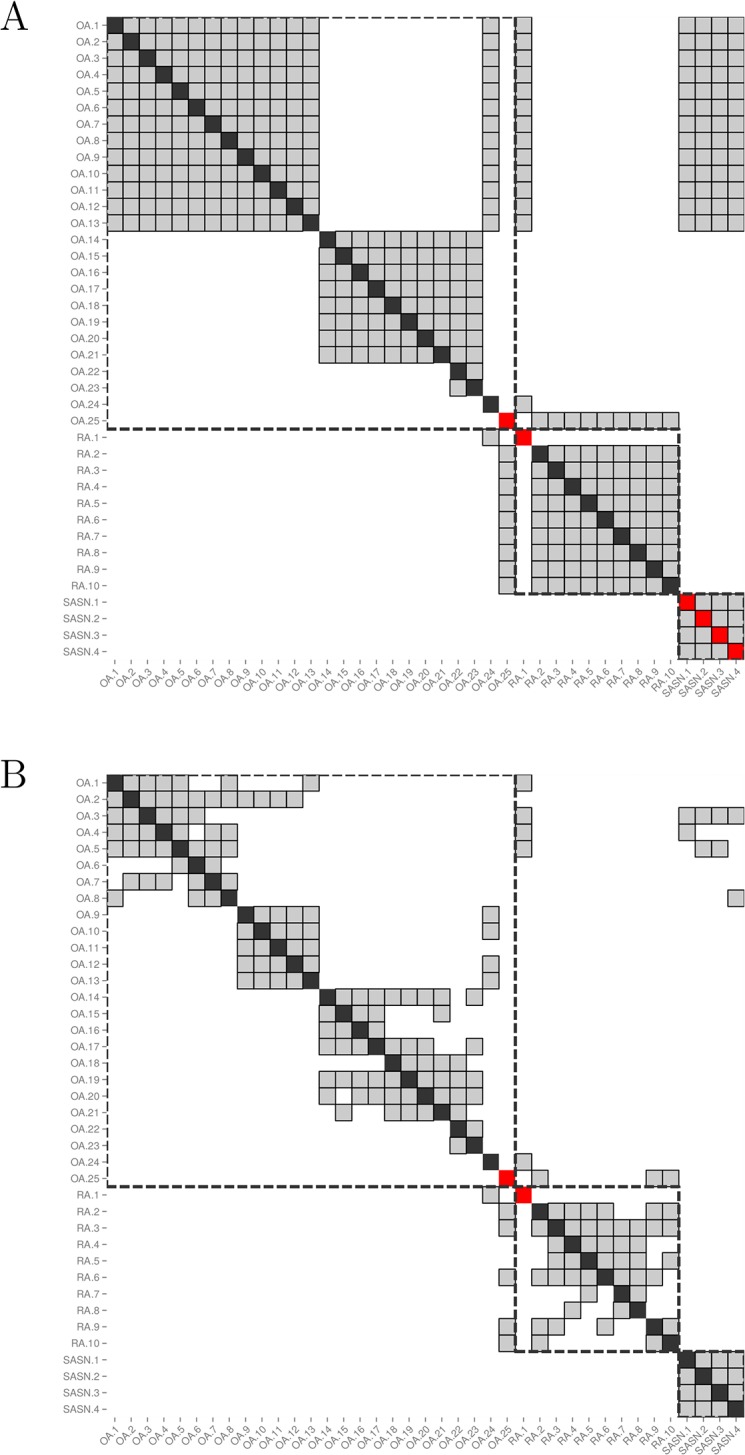
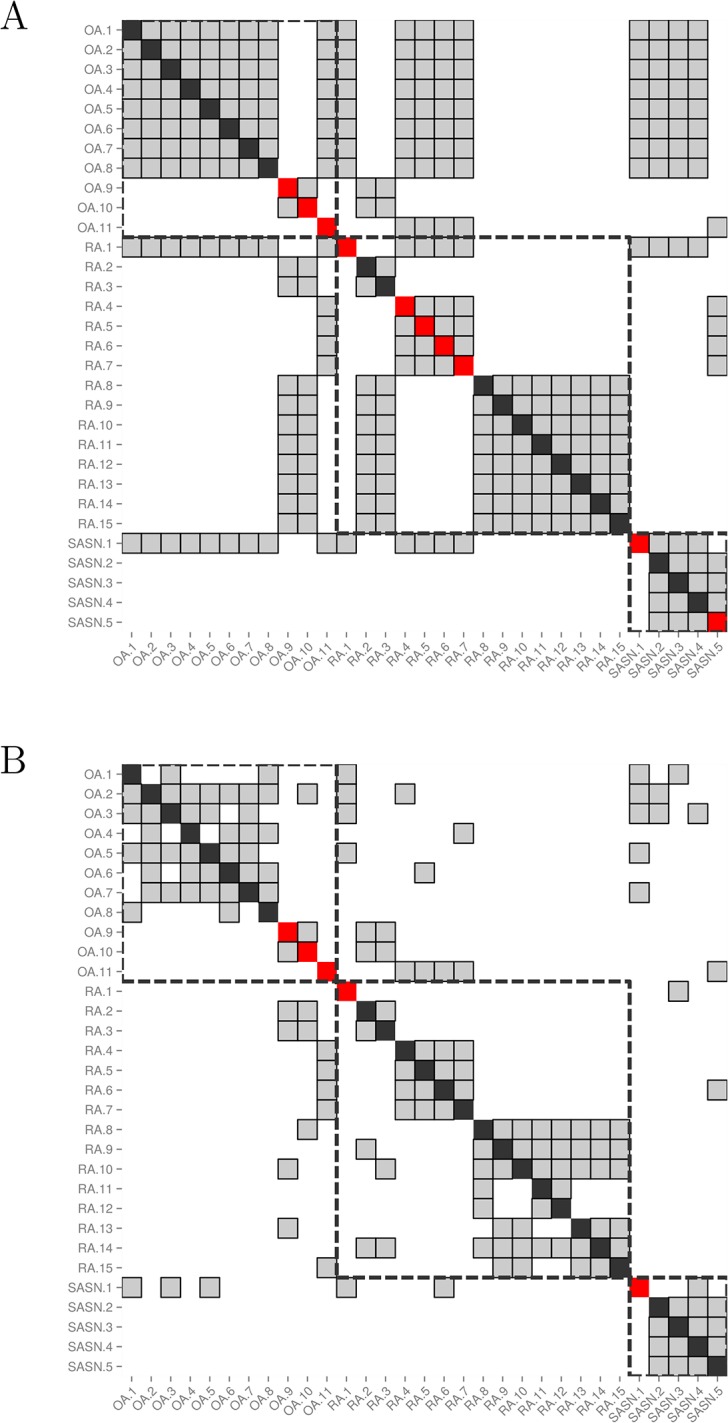
Results: According to high-density microarray data, several molecular pathways are differentially expressed in patients with RA, SA and OA: T and B cell activation, chromatin remodelling, RAS GTPase activation and extracellular matrix regulation. Strikingly, disease activity (DAS28-CRP) has a significant influence on gene expression patterns in RA samples. Using the low-density assays, samples from patients with OA are easily discriminated from RA and SA samples. However, overlapping molecular patterns are found, in particular between RA and SA biopsies. Therefore, prediction of the clinical diagnosis based on gene expression data results in a diagnostic accuracy of 56.8%, which is increased up to 98.6% by the addition of specific clinical symptoms in the prediction algorithm. Similar observations are made in initial UA samples, in which overlapping molecular patterns also impact the accuracy of the diagnostic algorithm. When clinical symptoms are added, the diagnostic accuracy is strongly improved.
Conclusions: Gene expression signatures are overall different in patients with OA, RA and SA, but overlapping molecular signatures are found in patients with these conditions. Therefore, an accurate diagnosis in patients with UA requires a combination of gene expression and clinical data.
Conflict of interest statement
Figures
References
-
- Quinn MA, Conaghan PG, Emery P. The therapeutic approach of early intervention for rheumatoid arthritis: what is the evidence? Rheumatology (Oxford). 2001; 40: 1211–20. - PubMed
-
- O’Dell JR. Treating rheumatoid arthritis early: a window of opportunity? Arthritis Rheum. 2002; 46: 283–5. - PubMed
-
- Mottonen T, Hannonen P, Korpela M, Nissilä M, Kautiainen H, Ilonen J, et al. FINnish Rheumatoid Arthritis Combination therapy. Delay to institution of therapy and induction of remission using single-drug or combination disease-modifying antirheumatic drug therapy in early rheumatoid arthritis. Arthritis Rheum. 2002; 46: 894–8. - PubMed
-
- Goekoop-Ruiterman YP, de Vries-Bouwstra JK, Allaart CF, van Zeben D, Kerstens PJ, Hazes JM, et al. Comparison of treatment strategies in early rheumatoid arthritis: a randomized trial. Ann Intern Med. 2007; 146: 406–15. - PubMed
-
- Emery P, McInnes IB, van Vollenhoven R, Kraan MC. Clinical identification and treatment of a rapidly progressing disease state in patients with rheumatoid arthritis. Rheumatology (Oxford). 2008; 47: 392–8. - PubMed
Publication types
MeSH terms
Associated data
- Actions
- Actions
- Actions
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
