

Time in blood glucose range 70 to 140 mg/dl >80% is strongly associated with increased survival in non-diabetic critically ill adults
- PMID: 25927986
- PMCID: PMC4446958
- DOI: 10.1186/s13054-015-0908-7
Time in blood glucose range 70 to 140 mg/dl >80% is strongly associated with increased survival in non-diabetic critically ill adults
Abstract
Introduction: Hyperglycemia, hypoglycemia and increased glucose variability are independently associated with increased risk of death in critically ill adults. The relationship between time in targeted blood glucose range (TIR) and mortality is not well described and may be a factor that has confounded the results of the major interventional trials of intensive insulin therapy.
Methods: We conducted a retrospective analysis of prospectively collected data involving 3,297 patients with intensive care unit (ICU) lengths of stay (LOS) of ≥ 1.0 day who were admitted between 1 January 2009 and 31 December 2013 to a single mixed medical-surgical ICU. We investigated the relationship between TIR 70 to 140 mg/dl with mortality and compared outcomes of non-diabetics (NON) and individuals with diabetes mellitus (DM), including stratifying by TIR above (TIR-hi) and below (TIR-lo) the median value for the NON and DM groups.
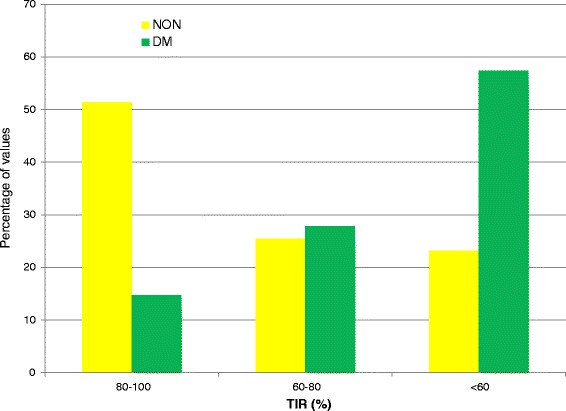
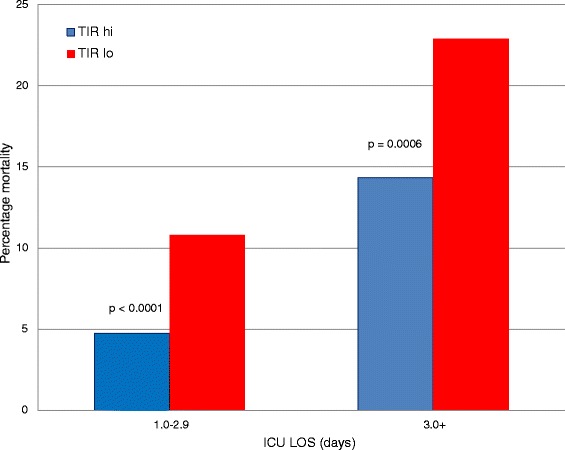
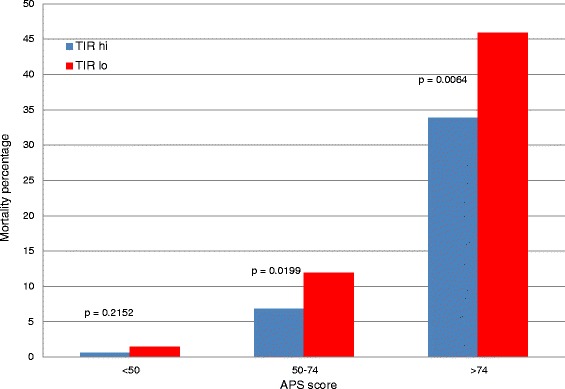
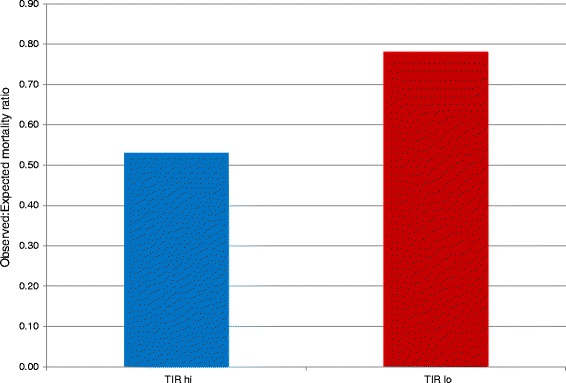
Results: There were 85,799 blood glucose (BG) values for the NON group and 32,651 for the DM group, and we found that 75.5% and 54.8%, respectively, were between 70 and 140 (P < 0.0001). The median (interquartile range) TIR (%) values for the NON and DM groups were 80.6% (61.4% to 94.0%) and 55.0% (35.5% to 71.1%), respectively (P < 0.0001). For the NON group, mortality was 8.47% and 15.71% for TIR-hi and TIR-lo, respectively (P < 0.0001). For the DM group, mortality was 16.09% and 14.44% for TIR-hi and TIR-lo, respectively (P = NS). We observed similar relationships for the NON group when we stratified by ICU LOS or severity of illness, especially in the most severely ill patients. There was a cumulative interaction of indices of hypoglycemia, hyperglycemia or glucose variability with TIR. Multivariable analysis demonstrated, for the NON group, that TIR-hi was independently associated with increased survival (P = 0.0019). For the NON group, the observed-to-expected mortality ratios for TIR-hi and TIR-lo, based on Acute Physiology and Chronic Health Evaluation IV methodology, were 0.53 and 0.78, respectively. In contrast, among those in the DM group, there was no clear relationship between TIR 70 to 140 mg/dl and survival.
Conclusions: Independently of ICU LOS and severity of illness, TIR 70 to 140 mg/dl > 80% is strongly associated with survival in critically ill patients without diabetes. These findings have implications for the design of clinical protocols for glycemic control in critically ill patients as well for the design of future interventional trials of intensive insulin therapy.
Figures
Comment in
-
Look at the patient--in sugar and infection.Crit Care. 2015 Dec 30;19:454. doi: 10.1186/s13054-015-1176-2. Crit Care. 2015. PMID: 26715534 Free PMC article. No abstract available.
Similar articles
-
Glucose control and mortality in critically ill patients.JAMA. 2003 Oct 15;290(15):2041-7. doi: 10.1001/jama.290.15.2041. JAMA. 2003. PMID: 14559958
-
Glucose Control, Diabetes Status, and Mortality in Critically Ill Patients: The Continuum From Intensive Care Unit Admission to Hospital Discharge.Mayo Clin Proc. 2017 Jul;92(7):1019-1029. doi: 10.1016/j.mayocp.2017.04.015. Epub 2017 Jun 20. Mayo Clin Proc. 2017. PMID: 28645517
-
Percentage of Time in Range 70 to 139 mg/dL Is Associated With Reduced Mortality Among Critically Ill Patients Receiving IV Insulin Infusion.Chest. 2019 Nov;156(5):878-886. doi: 10.1016/j.chest.2019.05.016. Epub 2019 Jun 12. Chest. 2019. PMID: 31201784
-
Glucose control in the intensive care unit.Crit Care Med. 2009 May;37(5):1769-76. doi: 10.1097/CCM.0b013e3181a19ceb. Crit Care Med. 2009. PMID: 19325461 Review.
-
The impact of premorbid diabetic status on the relationship between the three domains of glycemic control and mortality in critically ill patients.Curr Opin Clin Nutr Metab Care. 2012 Mar;15(2):151-60. doi: 10.1097/MCO.0b013e32834f0009. Curr Opin Clin Nutr Metab Care. 2012. PMID: 22234163 Review.
Cited by
-
3D kernel-density stochastic model for more personalized glycaemic control: development and in-silico validation.Biomed Eng Online. 2019 Oct 22;18(1):102. doi: 10.1186/s12938-019-0720-8. Biomed Eng Online. 2019. PMID: 31640720 Free PMC article.
-
Exogenous Ketones Lower Blood Glucose Level in Rested and Exercised Rodent Models.Nutrients. 2019 Oct 1;11(10):2330. doi: 10.3390/nu11102330. Nutrients. 2019. PMID: 31581549 Free PMC article.
-
Model-based glycemic control in a Malaysian intensive care unit: performance and safety study.Med Devices (Auckl). 2019 May 31;12:215-226. doi: 10.2147/MDER.S187840. eCollection 2019. Med Devices (Auckl). 2019. PMID: 31239792 Free PMC article.
-
Continuous glucose monitoring in the ICU: clinical considerations and consensus.Crit Care. 2017 Jul 31;21(1):197. doi: 10.1186/s13054-017-1784-0. Crit Care. 2017. PMID: 28756769 Free PMC article. Review.
-
Comparison of the efficacy and safety of insulin degludec/aspart (twice-daily injections), insulin glargine 300 U/mL, and insulin glulisine (basal-bolus therapy).J Diabetes Investig. 2019 Nov;10(6):1527-1536. doi: 10.1111/jdi.13038. Epub 2019 Apr 2. J Diabetes Investig. 2019. PMID: 30868726 Free PMC article. Clinical Trial.
References
-
- Preiser JC, Devos P, Ruiz-Santana S, Mélot C, Annane D, Groeneveld J, et al. A prospective randomised multi-centre controlled trial on tight glucose control by intensive insulin therapy in adult intensive care units: the Glucontrol study. Intensive Care Med. 2009;35:1738–48. doi: 10.1007/s00134-009-1585-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
