

Benefits and harms of mammography screening
- PMID: 25928287
- PMCID: PMC4415291
- DOI: 10.1186/s13058-015-0525-z
Benefits and harms of mammography screening
Abstract
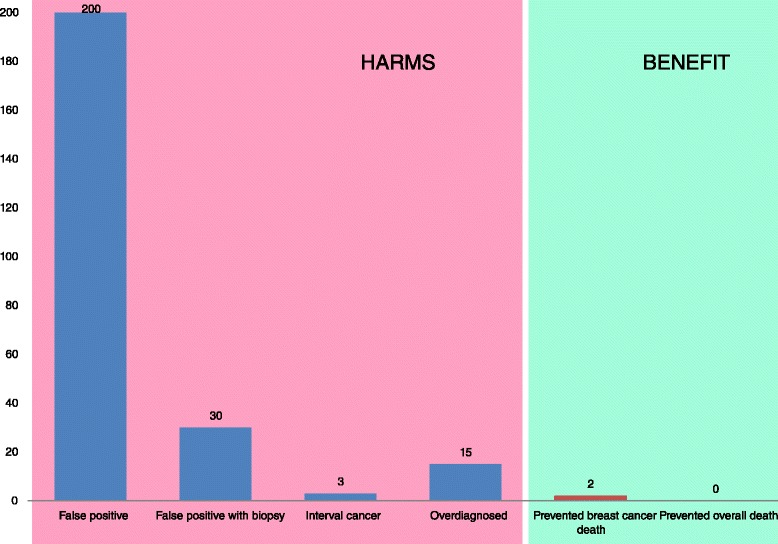
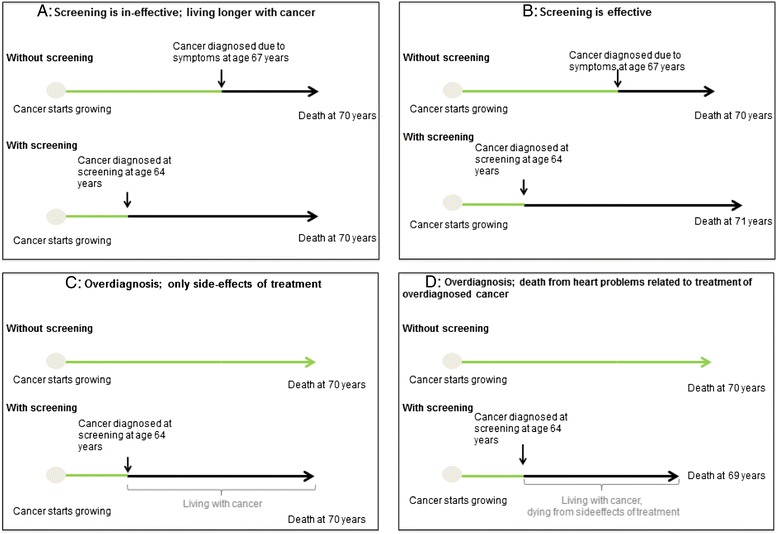
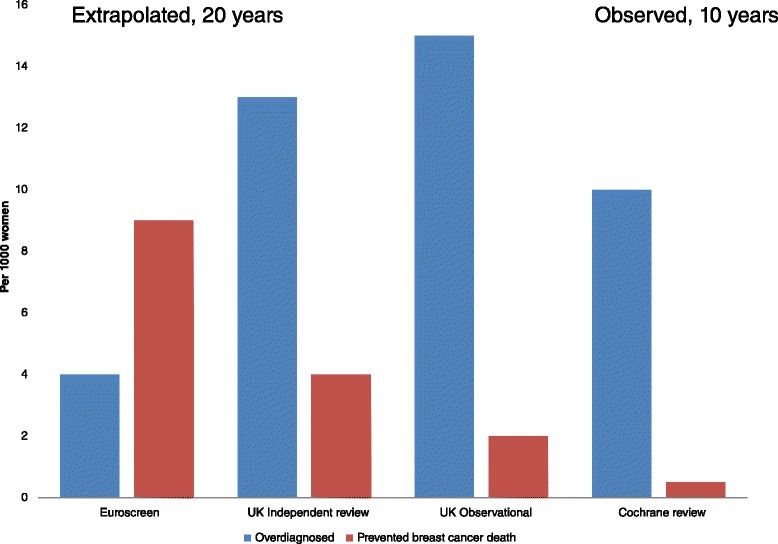
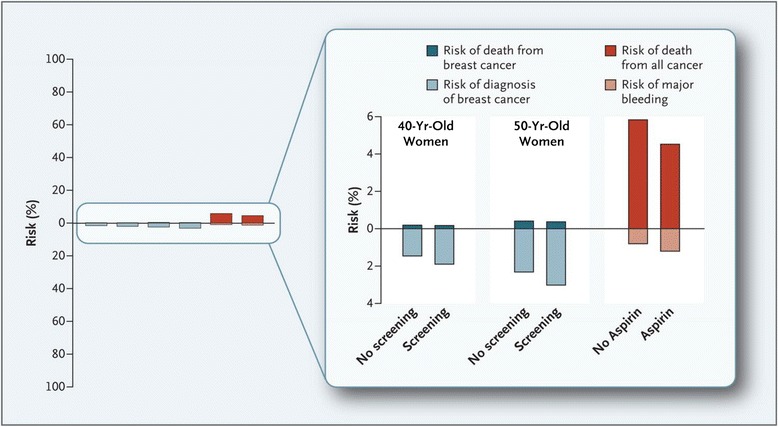
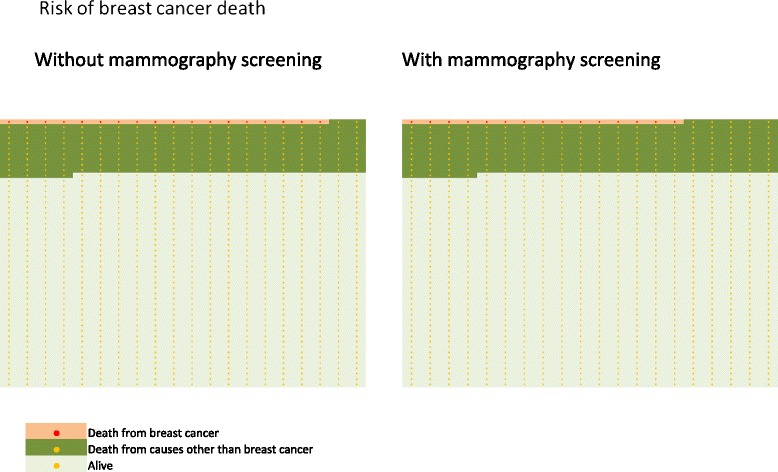
Mammography screening for breast cancer is widely available in many countries. Initially praised as a universal achievement to improve women's health and to reduce the burden of breast cancer, the benefits and harms of mammography screening have been debated heatedly in the past years. This review discusses the benefits and harms of mammography screening in light of findings from randomized trials and from more recent observational studies performed in the era of modern diagnostics and treatment. The main benefit of mammography screening is reduction of breast-cancer related death. Relative reductions vary from about 15 to 25% in randomized trials to more recent estimates of 13 to 17% in meta-analyses of observational studies. Using UK population data of 2007, for 1,000 women invited to biennial mammography screening for 20 years from age 50, 2 to 3 women are prevented from dying of breast cancer. All-cause mortality is unchanged. Overdiagnosis of breast cancer is the main harm of mammography screening. Based on recent estimates from the United States, the relative amount of overdiagnosis (including ductal carcinoma in situ and invasive cancer) is 31%. This results in 15 women overdiagnosed for every 1,000 women invited to biennial mammography screening for 20 years from age 50. Women should be unpassionately informed about the benefits and harms of mammography screening using absolute effect sizes in a comprehensible fashion. In an era of limited health care resources, screening services need to be scrutinized and compared with each other with regard to effectiveness, cost-effectiveness and harms.
Figures

References
-
- Shorter Oxford English Dictionary. Oxford, United Kingdom: Oxford University Press; 2010
-
- Raffle AE, Gray JAM. Screening: Evidence and Practice. Oxford, United Kingdom: Oxford University Press; 2007.
-
- Holland WW, Stewart S. Screening in Disease Prevention. What works? Oxford, United Kingdom: The Nuttfield Trust/Radcliffe Publishing Ltd; 2005.
-
- Wilson JMG, Junger G. Principles and Practice of Screening for Disease. Geneva, Switzerland: WHO; 1968.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
