

Evaluation of the PaO2/FiO2 ratio after cardiac surgery as a predictor of outcome during hospital stay
- PMID: 25928646
- PMCID: PMC4448284
- DOI: 10.1186/1471-2253-14-83
Evaluation of the PaO2/FiO2 ratio after cardiac surgery as a predictor of outcome during hospital stay
Abstract
Background: The arterial partial pressure of O2 and the fraction of inspired oxygen (PaO2/FiO2) ratio is widely used in ICUs as an indicator of oxygenation status. Although cardiac surgery and ICU scores can predict mortality, during the first hours after cardiac surgery few instruments are available to assess outcome. The aim of this study was to evaluate the usefulness of PaO2/FIO2 ratio to predict mortality in patients immediately after cardiac surgery.
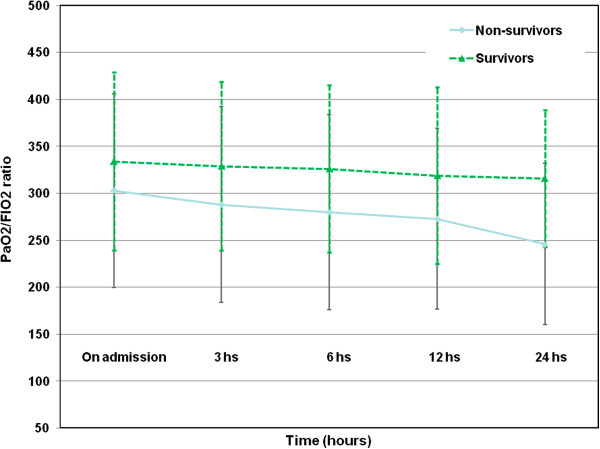
Methods: We prospectively studied 2725 consecutive cardiac surgery patients between 2004 and 2009. PaO2/FiO2 ratio was measured on admission and at 3 h, 6 h, 12 h and 24 h after ICU admission, together with clinical data and outcomes.
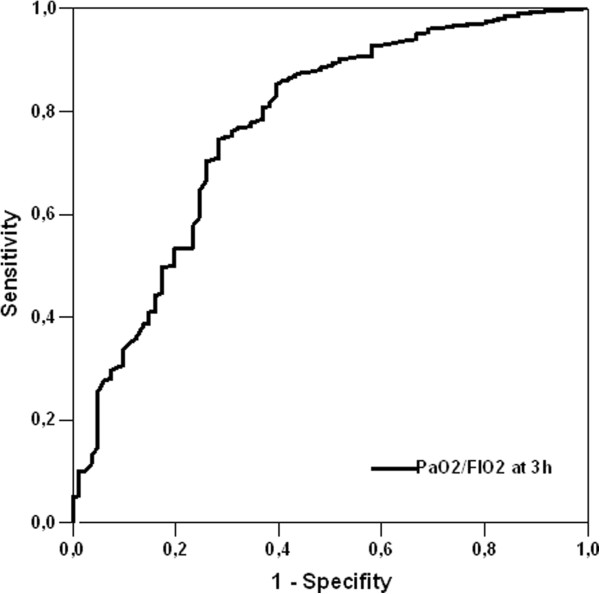
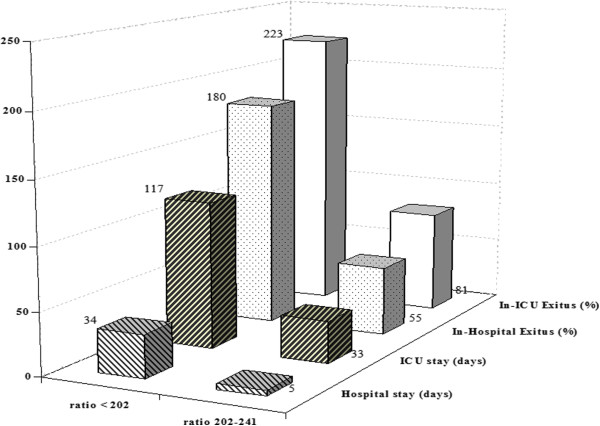
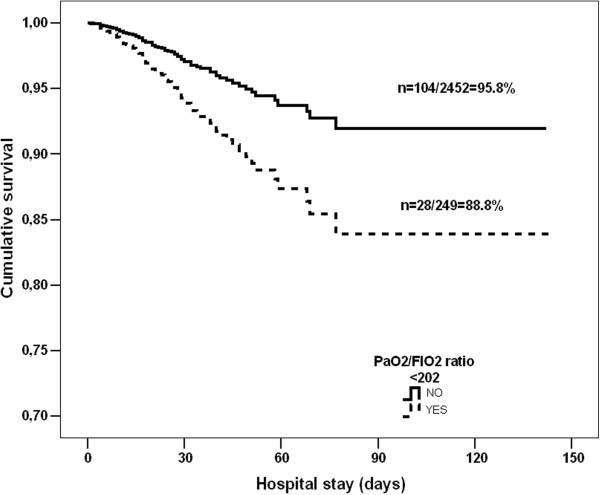
Results: All PaO2/FIO2 ratio measurements differed between survivors and non-survivors (p < 0.001). The PaO2/FIO2 at 3 h after ICU admission was the best predictor of mortality based on area under the curve (p < 0.001) and the optimum threshold estimation gave an optimal cut-off of 222 (95% Confidence interval (CI): 202-242), yielding three groups of patients: Group 1, with PaO2/FIO2 > 242; Group 2, with PaO2/FIO2 from 202 to 242; and Group 3, with PaO2/FIO2 < 202. Group 3 showed higher in-ICU mortality and ICU length of stay and Groups 2 and 3 also showed higher respiratory complication rates. The presence of a PaO2/FIO2 ratio < 202 at 3 h after admission was shown to be a predictor of in-ICU mortality (OR:1.364; 95% CI:1.212-1.625, p < 0.001) and of worse long-term survival (88.8% vs. 95.8%; Log rank p = 0.002. Adjusted Hazard ratio: 1.48; 95% CI:1.293-1.786; p = 0.004).
Conclusions: A simple determination of PaO2/FIO2 at 3 h after ICU admission may be useful to identify patients at risk immediately after cardiac surgery.
Figures
References
-
- Frutos-Vivar F, Nin N, Esteban A. Epidemiology of acute lung injury and acute respiratory distress syndrome. Curr Opin Crit Care. 2004;10:1–6. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
