

Variability of systemic and oro-dental phenotype in two families with non-lethal Raine syndrome with FAM20C mutations
- PMID: 25928877
- PMCID: PMC4422040
- DOI: 10.1186/s12881-015-0154-5
Variability of systemic and oro-dental phenotype in two families with non-lethal Raine syndrome with FAM20C mutations
Abstract
Background: Raine syndrome (RS) is a rare autosomal recessive bone dysplasia typified by osteosclerosis and dysmorphic facies due to FAM20C mutations. Initially reported as lethal in infancy, survival is possible into adulthood. We describe the molecular analysis and clinical phenotypes of five individuals from two consanguineous Brazilian families with attenuated Raine Syndrome with previously unreported features.
Methods: The medical and dental clinical records were reviewed. Extracted deciduous and permanent teeth as well as oral soft tissues were analysed. Whole exome sequencing was undertaken and FAM20C cDNA sequenced in family 1.
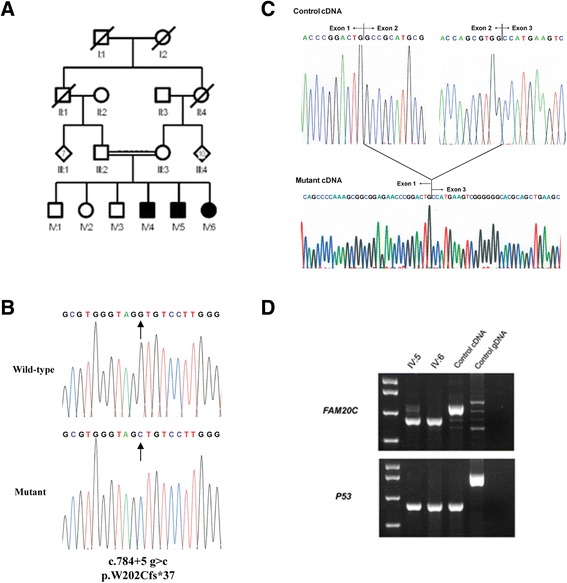
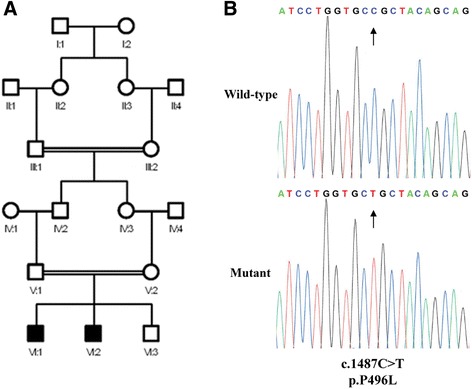
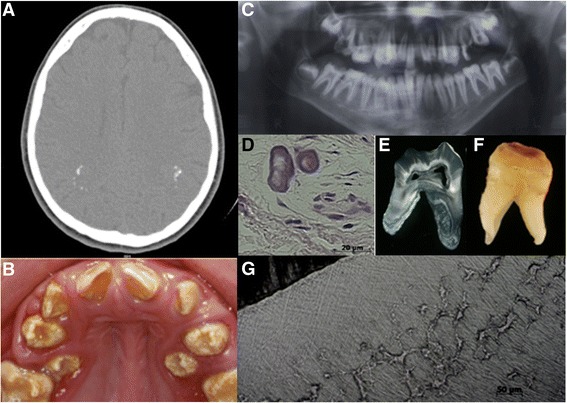
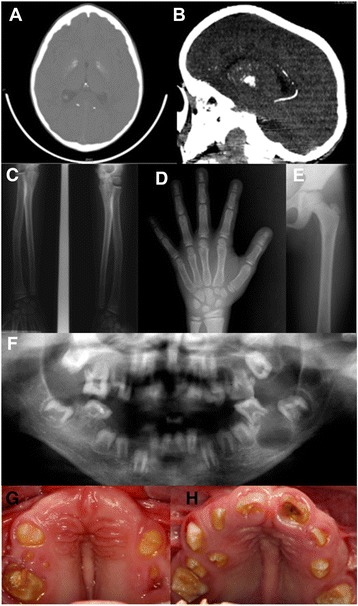
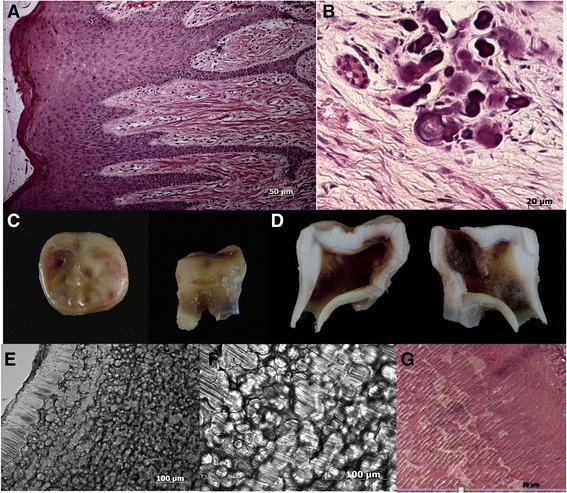
Results: Family 1 included 3 siblings with hypoplastic Amelogenesis Imperfecta (AI) (inherited abnormal dental enamel formation). Mild facial dysmorphism was noted in the absence of other obvious skeletal or growth abnormalities. A mild hypophosphataemia and soft tissue ectopic mineralization were present. A homozygous FAM20C donor splice site mutation (c.784 + 5 g > c) was identified which led to abnormal cDNA sequence. Family 2 included 2 siblings with hypoplastic AI and tooth dentine abnormalities as part of a more obvious syndrome with facial dysmorphism. There was hypophosphataemia, soft tissue ectopic mineralization, but no osteosclerosis. A homozygous missense mutation in FAM20C (c.1487C > T; p.P496L) was identified.
Conclusions: The clinical phenotype of non-lethal Raine Syndrome is more variable, including between affected siblings, than previously described and an adverse impact on bone growth and health may not be a prominent feature. By contrast, a profound failure of dental enamel formation leading to a distinctive hypoplastic AI in all teeth should alert clinicians to the possibility of FAM20C mutations.
Figures
References
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
