

The Bangladesh Risk of Acute Vascular Events (BRAVE) Study: objectives and design
- PMID: 25930055
- PMCID: PMC4516898
- DOI: 10.1007/s10654-015-0037-2
The Bangladesh Risk of Acute Vascular Events (BRAVE) Study: objectives and design
Abstract
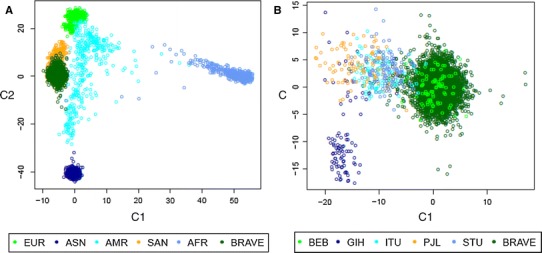
During recent decades, Bangladesh has experienced a rapid epidemiological transition from communicable to non-communicable diseases. Coronary heart disease (CHD), with myocardial infarction (MI) as its main manifestation, is a major cause of death in the country. However, there is limited reliable evidence about its determinants in this population. The Bangladesh Risk of Acute Vascular Events (BRAVE) study is an epidemiological bioresource established to examine environmental, genetic, lifestyle and biochemical determinants of CHD among the Bangladeshi population. By early 2015, the ongoing BRAVE study had recruited over 5000 confirmed first-ever MI cases, and over 5000 controls "frequency-matched" by age and sex. For each participant, information has been recorded on demographic factors, lifestyle, socioeconomic, clinical, and anthropometric characteristics. A 12-lead electrocardiogram has been recorded. Biological samples have been collected and stored, including extracted DNA, plasma, serum and whole blood. Additionally, for the 3000 cases and 3000 controls initially recruited, genotyping has been done using the CardioMetabochip+ and the Exome+ arrays. The mean age (standard deviation) of MI cases is 53 (10) years, with 88 % of cases being male and 46 % aged 50 years or younger. The median interval between reported onset of symptoms and hospital admission is 5 h. Initial analyses indicate that Bangladeshis are genetically distinct from major non-South Asian ethnicities, as well as distinct from other South Asian ethnicities. The BRAVE study is well-placed to serve as a powerful resource to investigate current and future hypotheses relating to environmental, biochemical and genetic causes of CHD in an important but under-studied South Asian population.
Figures
Similar articles
-
Cohort profile: the BangladEsh Longitudinal Investigation of Emerging Vascular and nonvascular Events (BELIEVE) cohort study.BMJ Open. 2025 Jan 22;15(1):e088338. doi: 10.1136/bmjopen-2024-088338. BMJ Open. 2025. PMID: 39843382 Free PMC article.
-
The Pakistan Risk of Myocardial Infarction Study: a resource for the study of genetic, lifestyle and other determinants of myocardial infarction in South Asia.Eur J Epidemiol. 2009;24(6):329-38. doi: 10.1007/s10654-009-9334-y. Epub 2009 Apr 30. Eur J Epidemiol. 2009. PMID: 19404752 Free PMC article.
-
Common and Rare Genetic Variation in CCR2, CCR5, or CX3CR1 and Risk of Atherosclerotic Coronary Heart Disease and Glucometabolic Traits.Circ Cardiovasc Genet. 2016 Jun;9(3):250-8. doi: 10.1161/CIRCGENETICS.115.001374. Epub 2016 Mar 24. Circ Cardiovasc Genet. 2016. PMID: 27013693 Free PMC article.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Increased unrecognized coronary heart disease and sudden deaths in rheumatoid arthritis: a population-based cohort study.Arthritis Rheum. 2005 Feb;52(2):402-11. doi: 10.1002/art.20853. Arthritis Rheum. 2005. PMID: 15693010 Review.
Cited by
-
Environmental toxic metal contaminants and risk of cardiovascular disease: systematic review and meta-analysis.BMJ. 2018 Aug 29;362:k3310. doi: 10.1136/bmj.k3310. BMJ. 2018. PMID: 30158148 Free PMC article.
-
Gene Sequencing Identifies Perturbation in Nitric Oxide Signaling as a Nonlipid Molecular Subtype of Coronary Artery Disease.Circ Genom Precis Med. 2022 Dec;15(6):e003598. doi: 10.1161/CIRCGEN.121.003598. Epub 2022 Oct 10. Circ Genom Precis Med. 2022. PMID: 36215124 Free PMC article.
-
Validation of a Genome-Wide Polygenic Score for Coronary Artery Disease in South Asians.J Am Coll Cardiol. 2020 Aug 11;76(6):703-714. doi: 10.1016/j.jacc.2020.06.024. J Am Coll Cardiol. 2020. PMID: 32762905 Free PMC article.
-
Transethnic Transferability of a Genome-Wide Polygenic Score for Coronary Artery Disease.Circ Genom Precis Med. 2021 Feb;14(1):e003092. doi: 10.1161/CIRCGEN.120.003092. Epub 2020 Dec 7. Circ Genom Precis Med. 2021. PMID: 33284643 Free PMC article. No abstract available.
-
Cohort profile: the BangladEsh Longitudinal Investigation of Emerging Vascular and nonvascular Events (BELIEVE) cohort study.BMJ Open. 2025 Jan 22;15(1):e088338. doi: 10.1136/bmjopen-2024-088338. BMJ Open. 2025. PMID: 39843382 Free PMC article.
References
-
- World Health Organization Global status report on noncommunicable diseases 2014. World Health Organization; 2015. - PubMed
-
- Leeder S, Raymond S, Greenberg H. A race against time: the challenge of cardiovascular disease in developing countries. New York: The Trustees of Columbia University in the city of New York; 2004.
-
- Naghavi M, Wang H, Lozano R, Davis A, Liang X, Zhou M, et al Global, regional, and national levels of age-sex specific all-cause and cause specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014; pii: S0140–6736(14)61682–2. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
