

Keratoconus: an inflammatory disorder?
- PMID: 25931166
- PMCID: PMC4506344
- DOI: 10.1038/eye.2015.63
Keratoconus: an inflammatory disorder?
Abstract
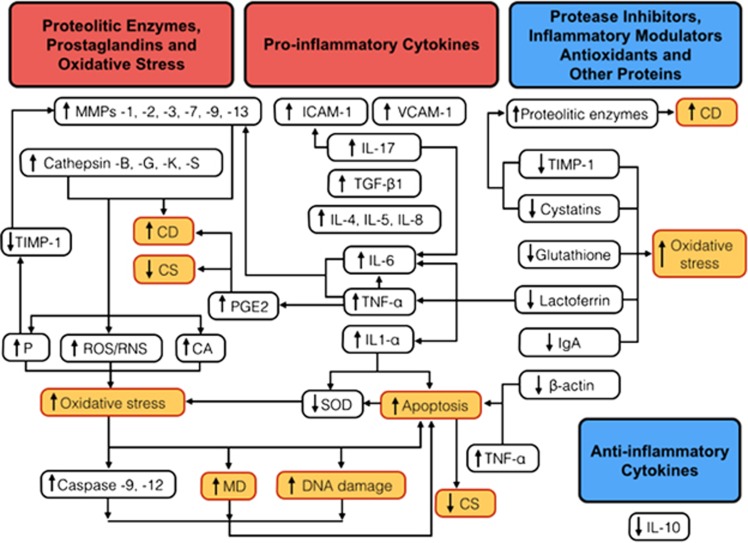
Keratoconus has been classically defined as a progressive, non-inflammatory condition, which produces a thinning and steepening of the cornea. Its pathophysiological mechanisms have been investigated for a long time. Both genetic and environmental factors have been associated with the disease. Recent studies have shown a significant role of proteolytic enzymes, cytokines, and free radicals; therefore, although keratoconus does not meet all the classic criteria for an inflammatory disease, the lack of inflammation has been questioned. The majority of studies in the tears of patients with keratoconus have found increased levels of interleukin-6 (IL-6), tumor necrosis factor-α(TNF-α), and matrix metalloproteinase (MMP)-9. Eye rubbing, a proven risk factor for keratoconus, has been also shown recently to increase the tear levels of MMP-13, IL-6, and TNF-α. In the tear fluid of patients with ocular rosacea, IL-1α and MMP-9 have been reported to be significantly elevated, and cases of inferior corneal thinning, resembling keratoconus, have been reported. We performed a literature review of published biochemical changes in keratoconus that would support that this could be, at least in part, an inflammatory condition.
Figures
Comment in
-
Reply.Cornea. 2017 Jan;36(1):e1-e2. doi: 10.1097/ICO.0000000000001053. Cornea. 2017. PMID: 27918358 No abstract available.
References
-
- Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42:297–319. - PubMed
-
- Krachmer JH, Feder RS, Belin MW. Keratoconus and related noninflammatory corneal thinning disorders. Surv Ophthalmol. 1984;28:293–322. - PubMed
-
- Brunsting LA, Reed WB, Bair HL. Occurrence of cataracts and keratoconus with atopic dermatitis. AMA Arch Derm. 1955;72:237–241. - PubMed
-
- Spencer WH, Fisher JJ. The association of keratoconus with atopic dermatitis. Am J Ophthalmol. 1959;47:332–344. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
