

Emerging therapies for patients with symptoms of opioid-induced bowel dysfunction
- PMID: 25931815
- PMCID: PMC4404965
- DOI: 10.2147/DDDT.S32684
Emerging therapies for patients with symptoms of opioid-induced bowel dysfunction
Abstract
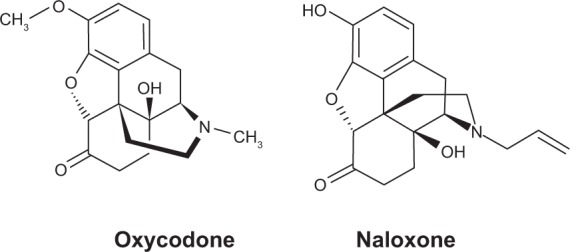
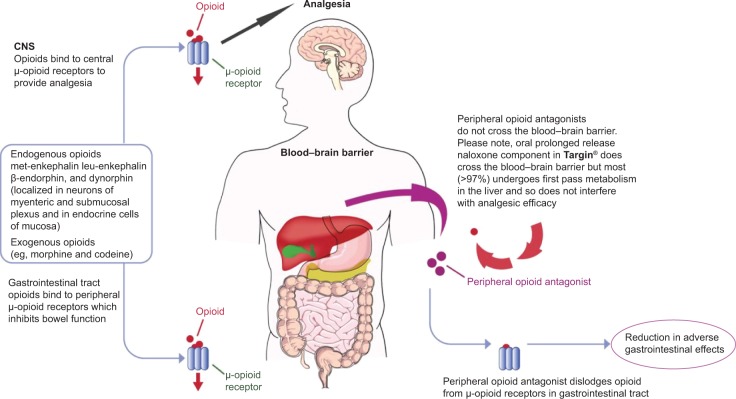
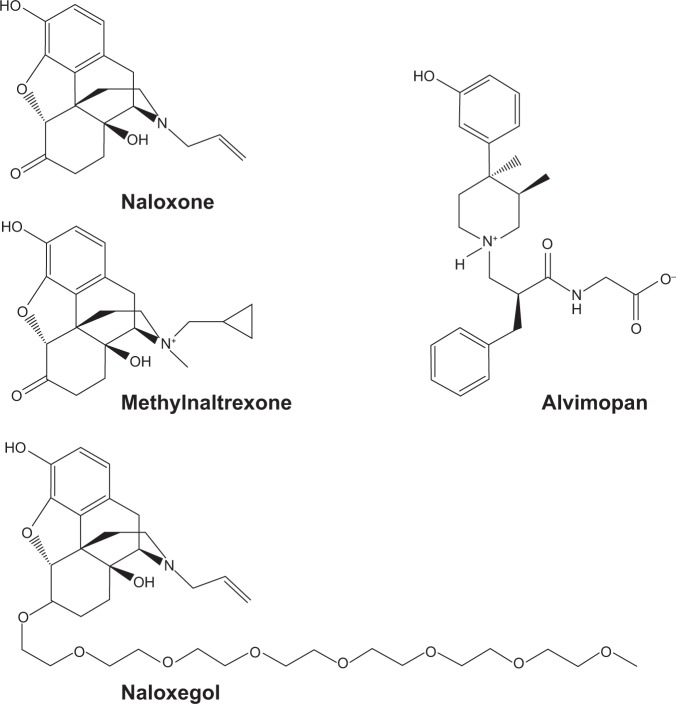
Opioid-induced bowel dysfunction (OIBD) comprises gastrointestinal (GI) symptoms, including dry mouth, nausea, vomiting, gastric stasis, bloating, abdominal pain, and opioid-induced constipation, which significantly impair patients' quality of life and may lead to undertreatment of pain. Traditional laxatives are often prescribed for OIBD symptoms, although they display limited efficacy and exert adverse effects. Other strategies include prokinetics and change of opioids or their administration route. However, these approaches do not address underlying causes of OIBD associated with opioid effects on mostly peripheral opioid receptors located in the GI tract. Targeted management of OIBD comprises purely peripherally acting opioid receptor antagonists and a combination of opioid receptor agonist and antagonist. Methylnaltrexone induces laxation in 50%-60% of patients with advanced diseases and OIBD who do not respond to traditional oral laxatives without inducing opioid withdrawal symptoms with similar response (45%-50%) after an oral administration of naloxegol. A combination of prolonged-release oxycodone with prolonged-release naloxone (OXN) in one tablet (a ratio of 2:1) provides analgesia with limited negative effect on the bowel function, as oxycodone displays high oral bioavailability and naloxone demonstrates local antagonist effect on opioid receptors in the GI tract and is totally inactivated in the liver. OXN in daily doses of up to 80 mg/40 mg provides equally effective analgesia with improved bowel function compared to oxycodone administered alone in patients with chronic non-malignant and cancer-related pain. OIBD is a common complication of long-term opioid therapy and may lead to quality of life deterioration and undertreatment of pain. Thus, a complex assessment and management that addresses underlying causes and patomechanisms of OIBD is recommended. Newer strategies comprise methylnaltrexone or OXN administration in the management of OIBD, and OXN may be also considered as a preventive measure of OIBD development in patients who require opioid administration.
Keywords: methylnaltrexone; naloxegol; opioid-induced bowel dysfunction; opioid-induced constipation; oxycodone/naloxone; quality of life.
Figures
Similar articles
-
Oxycodone/naloxone in the management of patients with pain and opioid-induced bowel dysfunction.Curr Drug Targets. 2014 Jan;15(1):124-35. doi: 10.2174/13894501113149990210. Curr Drug Targets. 2014. PMID: 24020972 Review.
-
The role of oxycodone/naloxone in the management of patients with pain and opioid-induced constipation.Expert Opin Pharmacother. 2019 Apr;20(5):511-522. doi: 10.1080/14656566.2018.1561863. Epub 2019 Jan 9. Expert Opin Pharmacother. 2019. PMID: 30625013 Review.
-
The role of naloxegol in the management of opioid-induced bowel dysfunction.Therap Adv Gastroenterol. 2016 Sep;9(5):736-46. doi: 10.1177/1756283X16648869. Epub 2016 May 26. Therap Adv Gastroenterol. 2016. PMID: 27582887 Free PMC article. Review.
-
The impact of opioid analgesics on the gastrointestinal tract function and the current management possibilities.Contemp Oncol (Pozn). 2012;16(2):125-31. doi: 10.5114/wo.2012.28792. Epub 2012 May 29. Contemp Oncol (Pozn). 2012. PMID: 23788866 Free PMC article.
-
Effects of prolonged-release oxycodone/naloxone on pain control, bowel function and quality of life: A prospective observational study.Scand J Pain. 2014 Apr 1;5(2):75-81. doi: 10.1016/j.sjpain.2014.01.004. Scand J Pain. 2014. PMID: 29913668
Cited by
-
Opioid-induced Constipation: Old and New Concepts in Diagnosis and Treatment.J Neurogastroenterol Motil. 2024 Apr 30;30(2):131-142. doi: 10.5056/jnm23144. J Neurogastroenterol Motil. 2024. PMID: 38576366 Free PMC article. Review.
-
Oxycodone/Naloxone Prolonged Release: A Review in Severe Chronic Pain.Clin Drug Investig. 2017 Dec;37(12):1191-1201. doi: 10.1007/s40261-017-0593-1. Clin Drug Investig. 2017. PMID: 29098567 Review.
-
Regulation of body weight and food intake by AGRP neurons during opioid dependence and abstinence in mice.Front Neural Circuits. 2022 Aug 30;16:977642. doi: 10.3389/fncir.2022.977642. eCollection 2022. Front Neural Circuits. 2022. PMID: 36110920 Free PMC article.
-
Pancreas Cancer-Associated Pain Management.Oncologist. 2021 Jun;26(6):e971-e982. doi: 10.1002/onco.13796. Epub 2021 May 12. Oncologist. 2021. PMID: 33885205 Free PMC article. Review.
-
Spotlight on naldemedine in the treatment of opioid-induced constipation in adult patients with chronic noncancer pain: design, development, and place in therapy.J Pain Res. 2018 Jan 15;11:195-199. doi: 10.2147/JPR.S141322. eCollection 2018. J Pain Res. 2018. PMID: 29391826 Free PMC article. Review.
References
-
- Cousins MJ, Lynch ME. The Declaration Montreal: access to pain management is a fundamental human right. Pain. 2011;152(12):2673–2674. - PubMed
-
- Knudsen AK, Brunelli C, Klepstad P, et al. Which domains should be included in a cancer pain classification system? Analyses of longitudinal data. Pain. 2012;153(3):696–703. - PubMed
-
- World Health Organisation . Cancer pain relief and palliative care. Geneva: World Health Organisation; 1996.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
