

Efficacy of the Osaka Medical College (OMC) brace in the treatment of adolescent idiopathic scoliosis following Scoliosis Research Society brace studies criteria
- PMID: 25932040
- PMCID: PMC4415349
- DOI: 10.1186/s13013-015-0036-9
Efficacy of the Osaka Medical College (OMC) brace in the treatment of adolescent idiopathic scoliosis following Scoliosis Research Society brace studies criteria
Abstract
Background: The efficacy of brace treatment for patients with adolescent idiopathic scoliosis (AIS) remains controversial. To make comparisons among studies more valid and reliable, the Scoliosis Research Society (SRS) has standardized criteria for brace studies in patients with AIS. The purpose of this study was to evaluate the efficacy of the Osaka Medical College (OMC) brace for AIS in accordance with the modified standardized criteria proposed by the SRS committee on bracing and non-operative management.
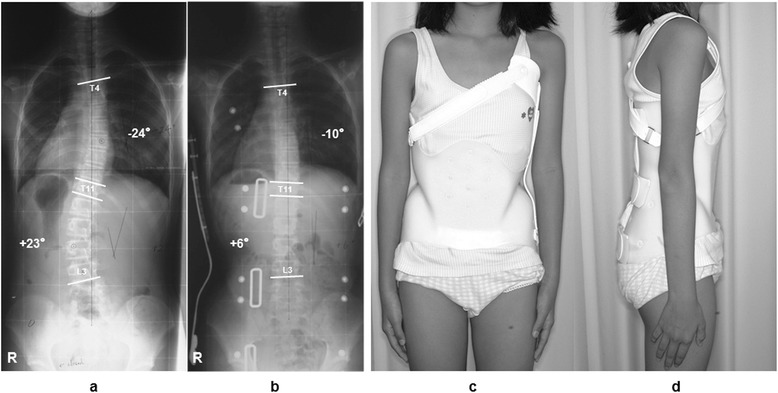
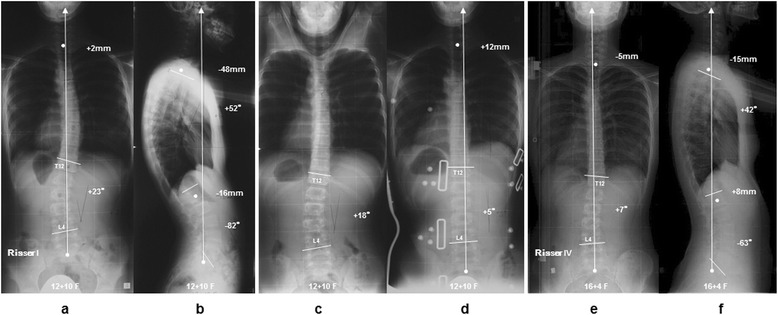
Methods: From 1999 through 2010, 31 consecutive patients with AIS who were newly prescribed the OMC brace and met the modified SRS criteria were studied. The study included 2 boys and 29 girls with a mean age of 12 years and 0 month. Patients were instructed to wear the brace for a minimum of 20 hours per day at the beginning of brace treatment. The mean duration of brace treatment was 4 years and 8 months. We examined the initial brace correction rate and the clinical outcomes of main curves evaluated by curve progression and surgical rate, and the compliance evaluated by the instruction adherence rate for all cases. The clinical course of the brace treatment was considered progression if ≥6° curvature increase occurred and improvement if ≥6° curvature decrease occurred according to SRS judgment criteria.
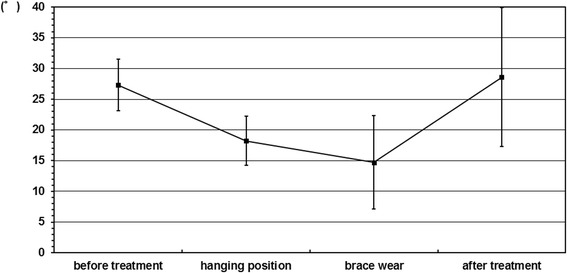
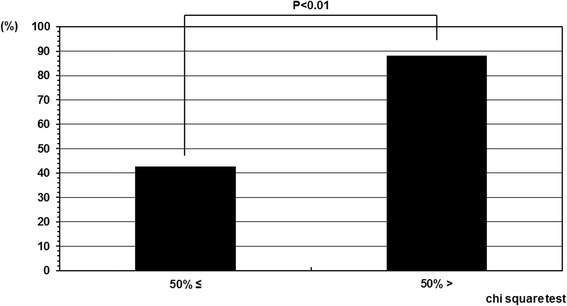
Results: The average initial brace correction rate was 46.8%. In 10 cases the curve progressed, 6 cases the curve improved, and 15 cases the curve remained unchanged (success rate: 67.7%). The mean instruction adherence rate, that was defined the percentage of the visits that patients declared they mostly followed our instruction to total visits, was 53.7%. The success rate was statistically higher in the patient group whose instruction adherence rate was greater than 50% (88.2%) as compared with in those 50% or less (42.8%).
Conclusions: OMC brace treatment for AIS patients could alter the natural history and significantly decreased the progression of curves to the threshold for surgical intervention. Better instruction adherence of brace wear associated with greater success.
Keywords: Adolescent idiopathic scoliosis (AIS); Conservative treatment; Hanging total spine x-ray; Osaka Medical College (OMC) brace; Scoliosis Research Society (SRS); Standardized inclusion and assessment criteria.
Figures
Similar articles
-
Predictive factors of Osaka Medical College (OMC) brace treatment in patients with adolescent idiopathic scoliosis.Scoliosis. 2015 Apr 10;10:11. doi: 10.1186/s13013-015-0038-7. eCollection 2015. Scoliosis. 2015. PMID: 25873992 Free PMC article.
-
The outcome of a modified version of the Cheneau brace in adolescent idiopathic scoliosis (AIS) based on SRS and SOSORT criteria: a retrospective study.Eur J Phys Rehabil Med. 2016 Oct;52(5):618-629. Epub 2016 May 4. Eur J Phys Rehabil Med. 2016. PMID: 27145218
-
A comparison of the thoracolumbosacral orthoses and providence orthosis in the treatment of adolescent idiopathic scoliosis: results using the new SRS inclusion and assessment criteria for bracing studies.J Pediatr Orthop. 2007 Jun;27(4):369-74. doi: 10.1097/01.bpb.0000271331.71857.9a. J Pediatr Orthop. 2007. PMID: 17513954
-
Standardization of criteria for adolescent idiopathic scoliosis brace studies: SRS Committee on Bracing and Nonoperative Management.Spine (Phila Pa 1976). 2005 Sep 15;30(18):2068-75; discussion 2076-7. doi: 10.1097/01.brs.0000178819.90239.d0. Spine (Phila Pa 1976). 2005. PMID: 16166897 Review.
-
Brace treatment in adolescent idiopathic scoliosis: risk factors for failure-a literature review.Spine J. 2019 Dec;19(12):1917-1925. doi: 10.1016/j.spinee.2019.07.008. Epub 2019 Jul 17. Spine J. 2019. PMID: 31325626 Review.
Cited by
-
Brace and Physiotherapeutic Scoliosis Specific Exercises (PSSE) for Adolescent Idiopathic Scoliosis (AIS) treatment: a prospective study following Scoliosis Research Society (SRS) criteria.Arch Physiother. 2022 Nov 1;12(1):22. doi: 10.1186/s40945-022-00150-5. Arch Physiother. 2022. PMID: 36316760 Free PMC article.
-
Global research hotspots and trends in non-surgical treatment of adolescent idiopathic scoliosis over the past three decades: a bibliometric and visualization study.Front Pediatr. 2024 Jan 10;11:1308889. doi: 10.3389/fped.2023.1308889. eCollection 2023. Front Pediatr. 2024. PMID: 38269292 Free PMC article.
-
Brace Treatment for Adolescent Idiopathic Scoliosis.J Clin Med. 2018 Jun 4;7(6):136. doi: 10.3390/jcm7060136. J Clin Med. 2018. PMID: 29867010 Free PMC article.
-
Impact of Rotation Correction after Brace Treatment on Prognosis in Adolescent Idiopathic Scoliosis.Asian Spine J. 2016 Oct;10(5):893-900. doi: 10.4184/asj.2016.10.5.893. Epub 2016 Oct 17. Asian Spine J. 2016. PMID: 27790317 Free PMC article.
-
Brace treatment for patients with scoliosis: State of the art.S Afr J Physiother. 2021 Oct 26;77(2):1573. doi: 10.4102/sajp.v77i2.1573. eCollection 2021. S Afr J Physiother. 2021. PMID: 34859162 Free PMC article.
References
-
- Cotrel Y, Dubousset J, Guilaumat M. New universal instrumentation in spinal surgery. Clin Orthop. 1988;227:10–23. - PubMed
-
- Asher MA, Strippgen WE, Heinig CF, Carson WL. Isola spinal implant system: principles, design, and applications. In: An HS, Cotler JM, editors. Spinal instrumentation. Baltimore, MD: Williams & Wilkins; 1992. pp. 325–51.
-
- Nachemson AL, Peterson LE. Effectiveness of treatment with a brace in girls who have adolescent idiopathic scoliosis. J Bone Joint Surg. 1995;77A:815–22. - PubMed
-
- Rowe DE, Bernstein SM, Riddick MF, Adler F, Emans JB, Gardner-Bonneau D. A meta-analysis of the efficacy of non-operative treatments for idiopathic scoliosis. J Bone Joint Surg. 1997;79A:664–74. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
