

Unexpected cause of a right hemiplegia secondary to the painless full-length aortic dissection: a case report and literature review
- PMID: 25932276
- PMCID: PMC4402923
Unexpected cause of a right hemiplegia secondary to the painless full-length aortic dissection: a case report and literature review
Abstract
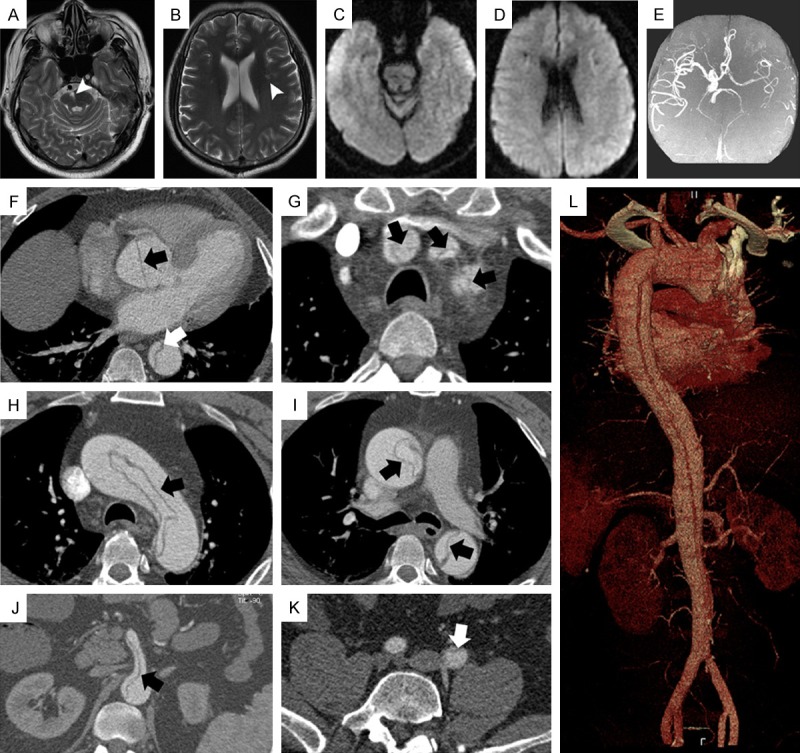
Painless aortic dissections in general are uncommon and are frequently misdiagnosed. Here we reported a rare case of acute ischemic stroke secondary to completely painless acute full-length dissection (DeBakey I) and provide a brief review of the literature. A 56-year-old man was referred to our department with right hemiplegia. Ischaemic stroke and thrombolytic treatment were considered initially. At the second examination, the patient was found to have decreased blood pressure, asymmetrical blood pressure/pulses between the bilateral limbs, and sudden loss of pulse in a lower extremity. Laboratory results revealed leucocytosis, elevated creatinine and CK without obvious cause. An aortic dissection was subsequently confirmed by contrast enhanced thoracic and abdominal CT scan. Our report provides some clues for the early diagnosis of painless aortic dissections.
Keywords: Completely painless acute aortic dissection; asymmetrical pulses; blood pressure; ischemic stroke.
Figures
References
-
- Estreicher M, Portale J, Lopez B. Aortic dissection presenting as gait disturbance: a case report. Am J Emerg Med. 2013;31:269, e261–262. - PubMed
-
- Gaul C, Dietrich W, Friedrich I, Sirch J, Erbguth FJ. Neurological symptoms in type A aortic dissections. Stroke. 2007;38:292–297. - PubMed
-
- Cohen S, Littmann D. Painless dissecting aneurysm of the aorta. N Engl J Med. 1964;271:143–5. - PubMed
-
- Rahmatullah SI, Khan IA, Nair VM, Caccavo ND, Vasavada BC, Sacchi TJ. Painless limited dissection of the ascending aorta presenting with aortic valve regurgitation. Am J Emerg Med. 1999;17:700–1. - PubMed
-
- Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122:311–28. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials