

Analyses Using Micro-CT Scans and Tissue Staining on New Bone Formation and Bone Fusion According to the Timing of Cranioplasty via Frozen Autologous Bone Flaps in Rabbits : A Preliminary Report
- PMID: 25932290
- PMCID: PMC4414767
- DOI: 10.3340/jkns.2015.57.4.242
Analyses Using Micro-CT Scans and Tissue Staining on New Bone Formation and Bone Fusion According to the Timing of Cranioplasty via Frozen Autologous Bone Flaps in Rabbits : A Preliminary Report
Abstract
Objective: The timing of cranioplasty and method of bone flap storage are known risk factors of non-union and resorption of bone flaps. In this animal experimental study, we evaluated the efficacy of cranioplasty using frozen autologous bone flap, and examined whether the timing of cranioplasty after craniectomy affects bone fusion and new bone formation.
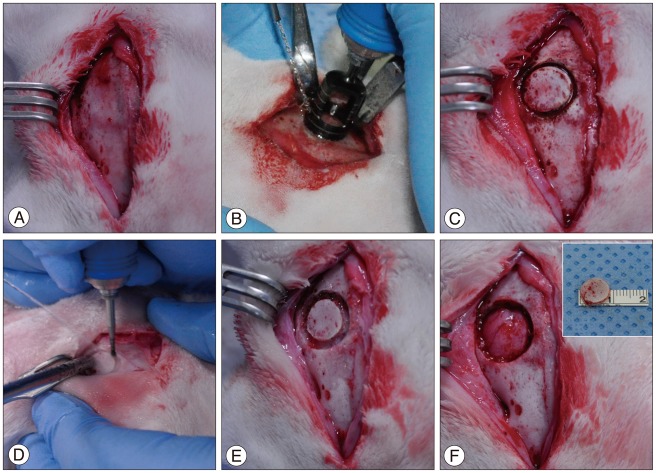
Methods: Total 8 rabbits (male, older than 16 weeks) were divided into two groups of early cranioplasty group (EG, 4 rabbits) and delayed cranioplasty group (DG, 4 rabbits). The rabbits of each group were performed cranioplasty via frozen autologous bone flaps 4 weeks (EG) and 8 weeks (DG) after craniectomy. In order to obtain control data, the cranioplasty immediate after craniectomy were made on the contralateral cranial bone of the rabbits (control group, CG).The bone fusion and new bone formation were evaluated by micro-CT scan and histological examination 8 weeks after cranioplasty on both groups.
Results: In the micro-CT scans, the mean values of the volume and the surface of new bone were 50.13±7.18 mm(3) and 706.23±77.26 mm(2) in EG, 53.78±10.86 mm(3) and 726.60±170.99 mm(2) in DG, and 31.51±12.84 mm(3) and 436.65±132.24 mm(2) in CG. In the statistical results, significant differences were shown between EG and CG and between DG and CG (volume : p=0.028 and surface : p=0.008). The histological results confirmed new bone formation in all rabbits.
Conclusion: We observed new bone formation on all the frozen autologous bone flaps that was stored within 8 weeks. The timing of cranioplasty may showed no difference of degree of new bone formation. Not only the healing period after cranioplasty but the time interval from craniectomy to cranioplasty could affect the new bone formation.
Keywords: Autologous bone; Cranioplasty; Frozen stored; Rabbits; Timing.
Figures





Similar articles
-
Long-term follow-up of cryopreservation with glycerol of autologous bone flaps for cranioplasty after decompressive craniectomy.Acta Neurochir (Wien). 2016 Mar;158(3):571-5. doi: 10.1007/s00701-015-2679-y. Epub 2016 Jan 6. Acta Neurochir (Wien). 2016. PMID: 26733129
-
The Fate of the Frozen Bone Flap: Quantitative and Volumetric Assessment Following Cranioplasty Using the Autologous Bone Flap.J Craniofac Surg. 2024 Dec 9. doi: 10.1097/SCS.0000000000010960. Online ahead of print. J Craniofac Surg. 2024. PMID: 39656195
-
Cranial autologous bone flap resorption after a cranioplasty: A case report.Surg Neurol Int. 2018 Mar 19;9:61. doi: 10.4103/sni.sni_388_17. eCollection 2018. Surg Neurol Int. 2018. PMID: 29629228 Free PMC article.
-
Delayed Cranioplasty: Outcomes Using Frozen Autologous Bone Flaps.Craniomaxillofac Trauma Reconstr. 2015 Sep;8(3):190-7. doi: 10.1055/s-0034-1395383. Epub 2014 Dec 17. Craniomaxillofac Trauma Reconstr. 2015. PMID: 26269726 Free PMC article.
-
Review of Cranioplasty after Decompressive Craniectomy.Korean J Neurotrauma. 2017 Apr;13(1):9-14. doi: 10.13004/kjnt.2017.13.1.9. Epub 2017 Apr 30. Korean J Neurotrauma. 2017. PMID: 28512612 Free PMC article. Review.
Cited by
-
X-ray micro-computed-tomography in pediatric surgery: a new tool for studying embryos.Pediatr Surg Int. 2018 Mar;34(3):297-305. doi: 10.1007/s00383-017-4213-1. Epub 2017 Nov 22. Pediatr Surg Int. 2018. PMID: 29167984
References
-
- Abbott KH. Use of frozen cranial bone flaps for autogenous and homologous grafts in cranioplasty and spinal interbody fusion. J Neurosurg. 1953;10:380–388. - PubMed
-
- Ahmadi SA, Meier U, Lemcke J. Detailed long-term outcome analysis after decompressive craniectomy for severe traumatic brain injury. Brain Inj. 2010;24:1539–1549. - PubMed
-
- Asano Y, Ryuke Y, Hasuo M, Simosawa S. [Cranioplasty using cryopreserved autogenous bone] No To Shinkei. 1993;45:1145–1150. - PubMed
-
- Chang V, Hartzfeld P, Langlois M, Mahmood A, Seyfried D. Outcomes of cranial repair after craniectomy. J Neurosurg. 2010;112:1120–1124. - PubMed
-
- Chibbaro S, Di Rocco F, Mirone G, Fricia M, Makiese O, Di Emidio P, et al. Decompressive craniectomy and early cranioplasty for the management of severe head injury : a prospective multicenter study on 147 patients. World Neurosurg. 2011;75:558–562. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
