

Guilt by association: paradigm for detecting a silent killer (thoracic aortic aneurysm)
- PMID: 25932333
- PMCID: PMC4410139
- DOI: 10.1136/openhrt-2014-000169
Guilt by association: paradigm for detecting a silent killer (thoracic aortic aneurysm)
Abstract
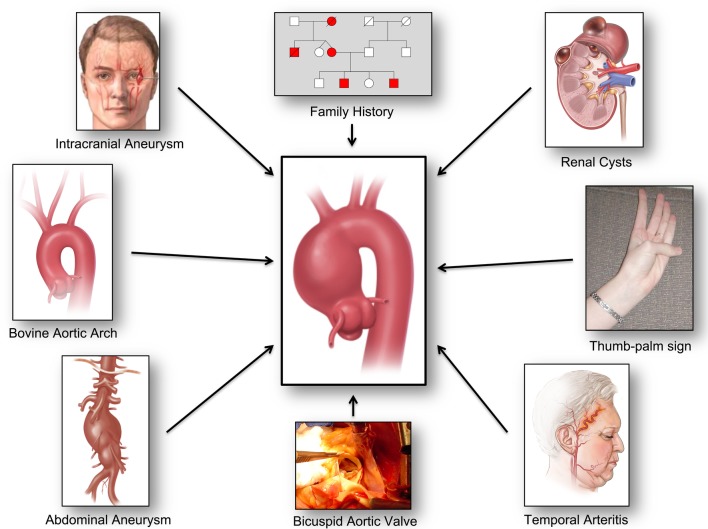
Recent studies have confirmed a close association between various medical conditions (intracranial aneurysm, abdominal aortic aneurysm, temporal arteritis, autoimmune disorder, renal cysts), certain aortic anatomic variants (bovine aortic arch, direct origin of left vertebral artery from aortic arch, bicuspid aortic valve), and family history of aneurysm disease with thoracic aortic aneurysm and dissection. This paper reviews these associations. We propose to capitalise on these associations as powerful and expanding opportunities to diagnose the virulent but silent disease of thoracic aortic aneurysm. This can be accomplished by recognition of this 'guilt by association' with the other conditions. Thus, patients with associated diseases and anatomic variants should be investigated for silent aortic aneurysms. Such a paradigm holds substantial potential for reducing death from the silent killer represented by thoracic aortic aneurysm disease.
Figures

References
-
- Elefteriades JA, Rizzo JA. Epidemiology: incidence, prevalence, and trends. In: Elefteriades JA. ed. Acute aortic disease. New York: Informa Healthcare, 2007:89–98.
-
- Centers for Disease Control. Twenty leading causes of death, United States 2010. All causes. All races, both sexes. http://webappa.cdc.gov/sasweb/ncipc/leadcaus10.html (accessed 17 Nov 2013).
-
- Elefteriades JA, Olin JW, Halperin JL. Diseases of the Aorta. In: Fuster V, ed.Hurst's the heart. 13th edn. New York: McGraw Hill, 2011:2261–89.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources