

Obstetric and neonatal outcomes after antipsychotic medication exposure in pregnancy
- PMID: 25932852
- PMCID: PMC4418034
- DOI: 10.1097/AOG.0000000000000759
Obstetric and neonatal outcomes after antipsychotic medication exposure in pregnancy
Abstract
Objective: Antipsychotic medications are used by increasing numbers of women of reproductive age. The safety of these medications during pregnancy has not been well described. We undertook a systematic review and meta-analysis of the adverse obstetric and neonatal outcomes associated with exposure to antipsychotics during pregnancy.
Data sources: PubMed, Reprotox, and ClinicalTrials.gov were searched to identify potential studies for inclusion.
Methods of study selection: Case-control or cohort studies estimating adverse birth outcomes associated with antipsychotic exposure during pregnancy were included. Pooled odds ratios (ORs) were used for dichotomous outcomes and weighted mean differences were used for neonatal birth weight and gestational age. Thirteen cohort studies, including 6,289 antipsychotic-exposed and 1,618,039 unexposed pregnancies, were included.
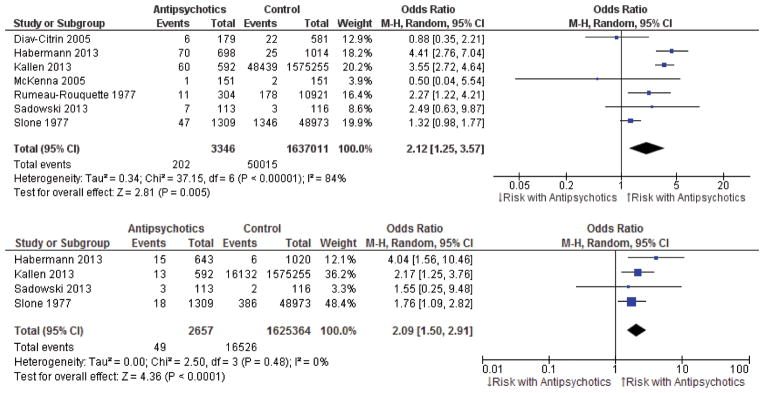
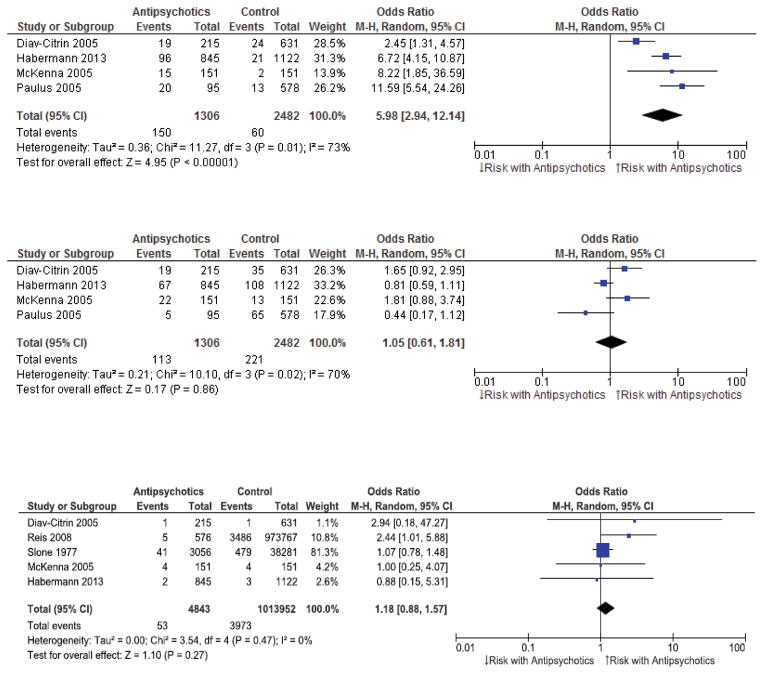
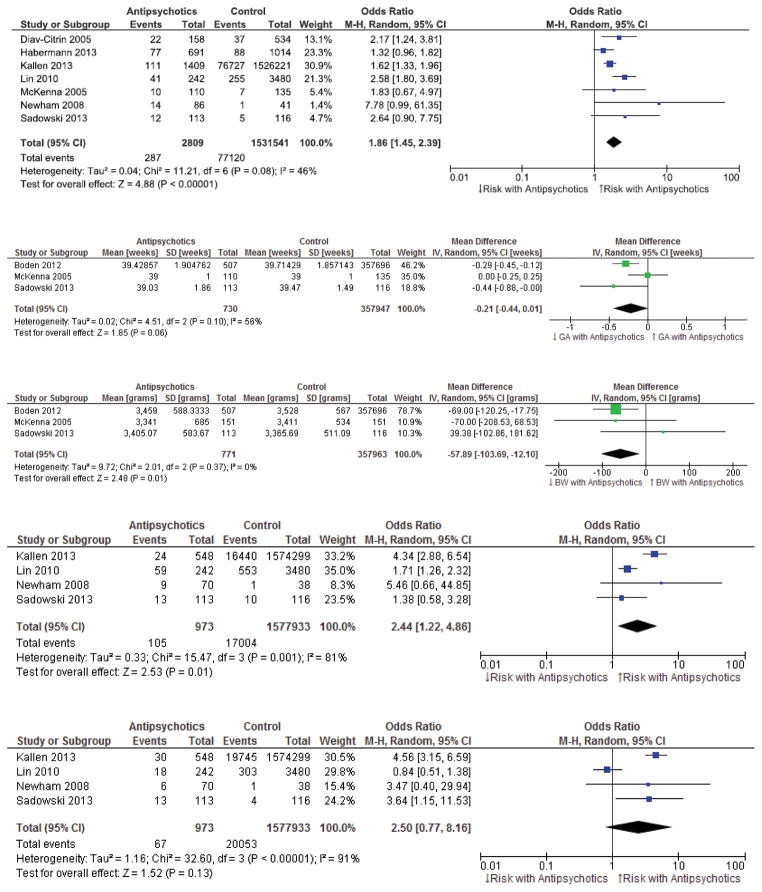
Tabulation, integration, and results: Antipsychotic exposure was associated with an increased risk of major malformations (absolute risk difference [ARD] 0.03, 95% confidence interval [CI] 0.00-0.05, P=.04, Z=2.06), heart defects (ARD 0.01, 95% CI 0.00-0.01, P<.001, Z=3.44), preterm delivery (ARD 0.05, 95% CI 0.03-0.08, P<.001, Z=4.10), small-for-gestational-age births (ARD 0.05, 95% CI 0.02-0.09, P=.006, Z=2.74), elective termination (ARD 0.09, 95% CI 0.05-0.13, P<.001, Z=4.69), and decreased birth weight (weighted mean difference -57.89 g, 95% CI -103.69 to -12.10 g, P=.01). There was no significant difference in the risk of major malformations (test for subgroup differences: χ²=0.07, degrees of freedom=1, P=.79) between typical (OR 1.55, 95% CI 1.21-1.99, P=.006) and atypical (OR 1.39, 95% CI 0.66-2.93, P=.38) antipsychotic medications. Antipsychotic exposure was not associated with risk of large-for-gestational-age births, stillbirth, and spontaneous abortion. Although antipsychotic exposure during pregnancy was associated with increased risk of adverse obstetric and neonatal outcomes, this association does not necessarily imply causation. This analysis was limited by the small number of included studies and limited adjustment in studies for possible confounders.
Conclusion: Women requiring antipsychotic treatment during pregnancy appear at higher risk of adverse birth outcomes, regardless of causation, and may benefit from close monitoring and minimization of other potential risk factors during pregnancy.
Figures
Similar articles
-
Metformin for women who are overweight or obese during pregnancy for improving maternal and infant outcomes.Cochrane Database Syst Rev. 2018 Jul 24;7(7):CD010564. doi: 10.1002/14651858.CD010564.pub2. Cochrane Database Syst Rev. 2018. PMID: 30039871 Free PMC article.
-
Antenatal dietary education and supplementation to increase energy and protein intake.Cochrane Database Syst Rev. 2015 Jun 2;(6):CD000032. doi: 10.1002/14651858.CD000032.pub3. Cochrane Database Syst Rev. 2015. PMID: 26031211
-
Treating periodontal disease for preventing adverse birth outcomes in pregnant women.Cochrane Database Syst Rev. 2017 Jun 12;6(6):CD005297. doi: 10.1002/14651858.CD005297.pub3. Cochrane Database Syst Rev. 2017. PMID: 28605006 Free PMC article.
-
Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour.Cochrane Database Syst Rev. 2015 Dec 14;2015(12):CD011200. doi: 10.1002/14651858.CD011200.pub2. Cochrane Database Syst Rev. 2015. PMID: 26662716 Free PMC article.
-
Ethanol for preventing preterm birth in threatened preterm labor.Cochrane Database Syst Rev. 2015 Nov 5;2015(11):CD011445. doi: 10.1002/14651858.CD011445.pub2. Cochrane Database Syst Rev. 2015. PMID: 26544539 Free PMC article.
Cited by
-
Does Gender Influence Outcome in Schizophrenia?Psychiatr Q. 2019 Mar;90(1):173-184. doi: 10.1007/s11126-018-9619-y. Psychiatr Q. 2019. PMID: 30484001 Review.
-
Neurodevelopment in school-aged children after intrauterine exposure to antipsychotics.Acta Psychiatr Scand. 2023 Jan;147(1):43-53. doi: 10.1111/acps.13517. Epub 2022 Nov 10. Acta Psychiatr Scand. 2023. PMID: 36333825 Free PMC article.
-
Prenatal exposure to antipsychotic medication and use of primary health care system in childhood: a population-based cohort study in Denmark.Clin Epidemiol. 2017 Dec 1;9:657-666. doi: 10.2147/CLEP.S145524. eCollection 2017. Clin Epidemiol. 2017. PMID: 29238228 Free PMC article.
-
Selective Serotonin Reuptake Inhibitor (SSRI) Antidepressants in Pregnancy and Congenital Anomalies: Analysis of Linked Databases in Wales, Norway and Funen, Denmark.PLoS One. 2016 Dec 1;11(12):e0165122. doi: 10.1371/journal.pone.0165122. eCollection 2016. PLoS One. 2016. PMID: 27906972 Free PMC article.
-
Depression and Anxiety During Pregnancy: Evaluating the Literature in Support of Clinical Risk-Benefit Decision-Making.Curr Psychiatry Rep. 2016 Jun;18(6):59. doi: 10.1007/s11920-016-0698-x. Curr Psychiatry Rep. 2016. PMID: 27091646 Review.
References
-
- Einarson A, Boskovic R. Use and safety of antipsychotic drugs during pregnancy. Journal of psychiatric practice. 2009 May;15(3):183–92. - PubMed
-
- Howard LM. Fertility and pregnancy in women with psychotic disorders. European journal of obstetrics, gynecology, and reproductive biology. 2005 Mar 1;119(1):3–10. - PubMed
-
- McCauley-Elsom K, Gurvich C, Elsom SJ, Kulkarni J. Antipsychotics in pregnancy. Journal of psychiatric and mental health nursing. 2010 Mar;17(2):97–104. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
