

3D-manufactured patient-specific models of congenital heart defects for communication in clinical practice: feasibility and acceptability
- PMID: 25933810
- PMCID: PMC4420970
- DOI: 10.1136/bmjopen-2014-007165
3D-manufactured patient-specific models of congenital heart defects for communication in clinical practice: feasibility and acceptability
Abstract
Objectives: To assess the communication potential of three-dimensional (3D) patient-specific models of congenital heart defects and their acceptability in clinical practice for cardiology consultations.
Design: This was a questionnaire-based study in which participants were randomised into two groups: the 'model group' received a 3D model of the cardiac lesion(s) being discussed during their appointment, while the 'control group' had a routine visit.
Setting: Outpatient clinic, cardiology follow-up visits.
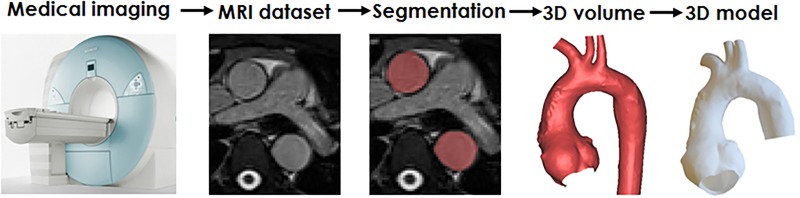
Participants: 103 parents of children with congenital heart disease were recruited (parental age: 43±8 years; patient age: 12±6 years). In order to have a 3D model made, patients needed to have a recent cardiac MRI examination; this was the crucial inclusion criterion.
Interventions: Questionnaires were administered to the participants before and after the visits and an additional questionnaire was administered to the attending cardiologist.
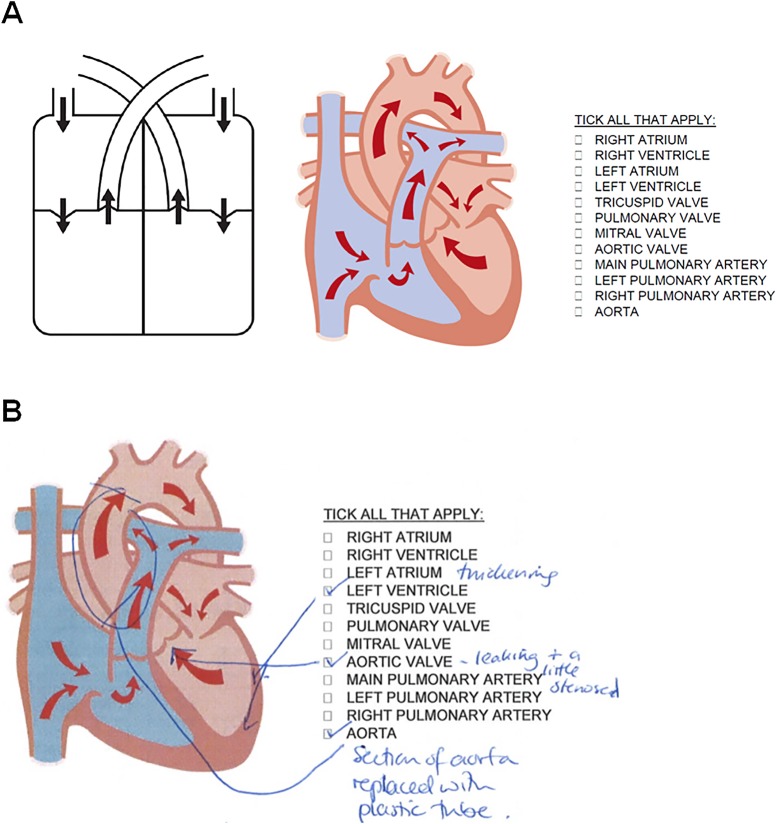
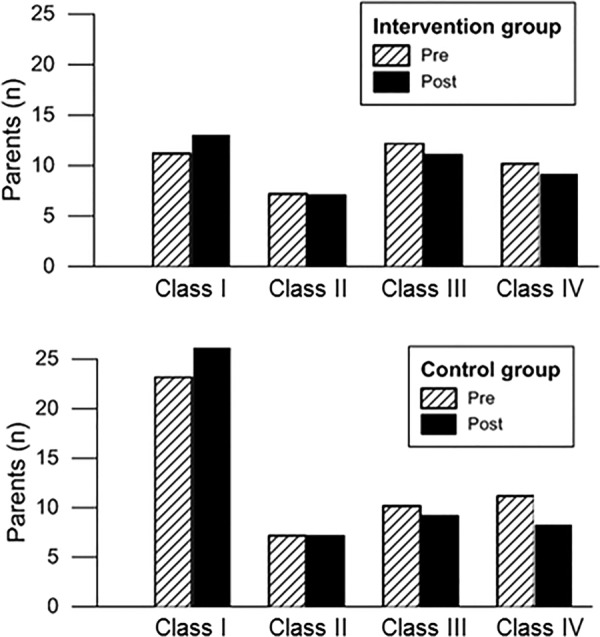
Main outcome measures: Rating (1-10) for the liking of the 3D model, its usefulness and the clarity of the explanation received were recorded, as well as rating (1-10) of the parental understanding and their engagement according to the cardiologist. Furthermore, parental knowledge was assessed by asking them to mark diagrams, tick keywords and provide free text answers. The duration of consultations was recorded and parent feedback collected.
Results: Parents and cardiologists both found the models to be very useful and helpful in engaging the parents in discussing congenital heart defects. Parental knowledge was not associated with their level of education (p=0.2) and did not improve following their visit. Consultations involving 3D models lasted on average 5 min longer (p=0.02).
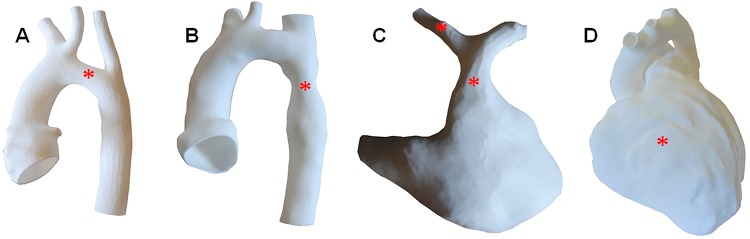
Conclusions: Patient-specific models can enhance engagement with parents and improve communication between cardiologists and parents, potentially impacting on parent and patient psychological adjustment following treatment. However, in the short-term, parental understanding of their child's condition did not improve.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
Similar articles
-
Piloting the Use of Patient-Specific Cardiac Models as a Novel Tool to Facilitate Communication During Cinical Consultations.Pediatr Cardiol. 2017 Apr;38(4):813-818. doi: 10.1007/s00246-017-1586-9. Epub 2017 Feb 18. Pediatr Cardiol. 2017. PMID: 28214968 Free PMC article.
-
Opening Pandora's box: parental anxiety and the assessment of childhood murmurs.Can J Cardiol. 2002 Apr;18(4):406-14. Can J Cardiol. 2002. PMID: 11992134
-
"You Have to Find a Way for This Child to Be at the Center": Pediatric Cardiologists' Views on Triadic Communication in Consultations on Congenital Heart Defects.Health Commun. 2025 Jan;40(1):15-26. doi: 10.1080/10410236.2024.2329422. Epub 2024 Apr 1. Health Commun. 2025. PMID: 38557305
-
Three-dimensional printing and virtual surgery for congenital heart procedural planning.Birth Defects Res. 2018 Aug 1;110(13):1082-1090. doi: 10.1002/bdr2.1370. Epub 2018 Aug 6. Birth Defects Res. 2018. PMID: 30079634 Review.
-
Three-dimensional Printed Cardiac Models: Applications in the Field of Medical Education, Cardiovascular Surgery, and Structural Heart Interventions.Rev Esp Cardiol (Engl Ed). 2017 Apr;70(4):282-291. doi: 10.1016/j.rec.2017.01.012. Epub 2017 Feb 8. Rev Esp Cardiol (Engl Ed). 2017. PMID: 28189544 Review. English, Spanish.
Cited by
-
Application of Three-Dimensional Printing Technology in the Perioperative Management of Cardiac Tumours: A Review and Analysis.Rev Cardiovasc Med. 2024 Mar 11;25(3):101. doi: 10.31083/j.rcm2503101. eCollection 2024 Mar. Rev Cardiovasc Med. 2024. PMID: 39076958 Free PMC article.
-
Assessment of post-infarct ventricular septal defects through 3D printing and statistical shape analysis.J 3D Print Med. 2023 Mar;7(1):3DP3. doi: 10.2217/3dp-2022-0012. Epub 2023 Jan 18. J 3D Print Med. 2023. PMID: 36911812 Free PMC article.
-
3D printing in medicine of congenital heart diseases.3D Print Med. 2015;2(1):3. doi: 10.1186/s41205-016-0004-x. Epub 2016 Sep 13. 3D Print Med. 2015. PMID: 30050975 Free PMC article. Review.
-
Augmented Reality Visualization of 3D Rotational Angiography in Congenital Heart Disease: A Comparative Study to Standard Computer Visualization.Pediatr Cardiol. 2024 Dec;45(8):1759-1766. doi: 10.1007/s00246-023-03278-8. Epub 2023 Sep 19. Pediatr Cardiol. 2024. PMID: 37725124
-
Personalized Three-Dimensional Printed Models in Congenital Heart Disease.J Clin Med. 2019 Apr 16;8(4):522. doi: 10.3390/jcm8040522. J Clin Med. 2019. PMID: 30995803 Free PMC article. Review.
References
-
- Harris J, Rimmell J. Can rapid prototyping ever become a routine feature in general dental practice? Dent Update 2002;29:482–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical