

Metformin increases survival in hormone receptor-positive, HER2-positive breast cancer patients with diabetes
- PMID: 25935404
- PMCID: PMC4504447
- DOI: 10.1186/s13058-015-0574-3
Metformin increases survival in hormone receptor-positive, HER2-positive breast cancer patients with diabetes
Abstract
Introduction: Metformin use has recently been observed to decrease both the rate and mortality of breast cancer. Our study was aim to determine whether metformin use is associated with survival in diabetic breast cancer patients by breast cancer subtype and systemic treatment.
Methods: Data from the Asan Medical Center Breast Cancer Database from 1997 to 2007 were analyzed. The study cohort comprised 6,967 nondiabetic patients, 202 diabetic patients treated with metformin, and 184 diabetic patients that did not receive metformin. Patients who were divided into three groups by diabetes status and metformin use were also divided into four subgroups by hormone receptor and HER2-neu status.
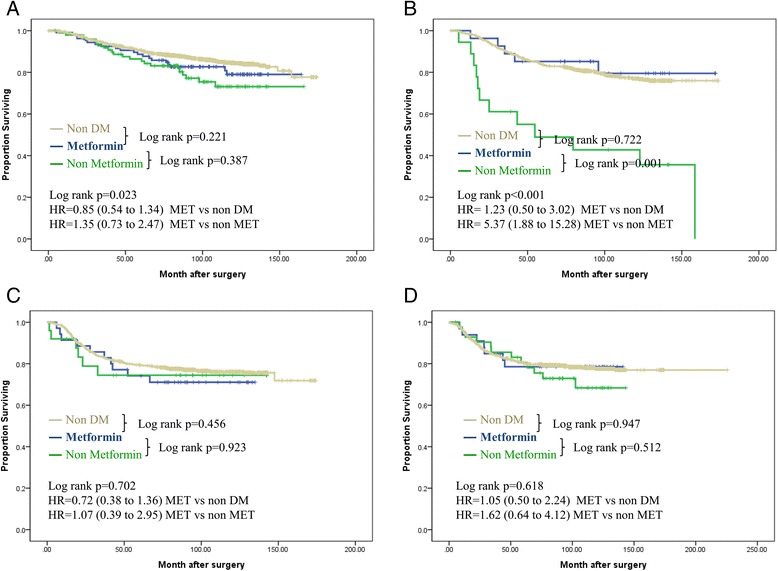
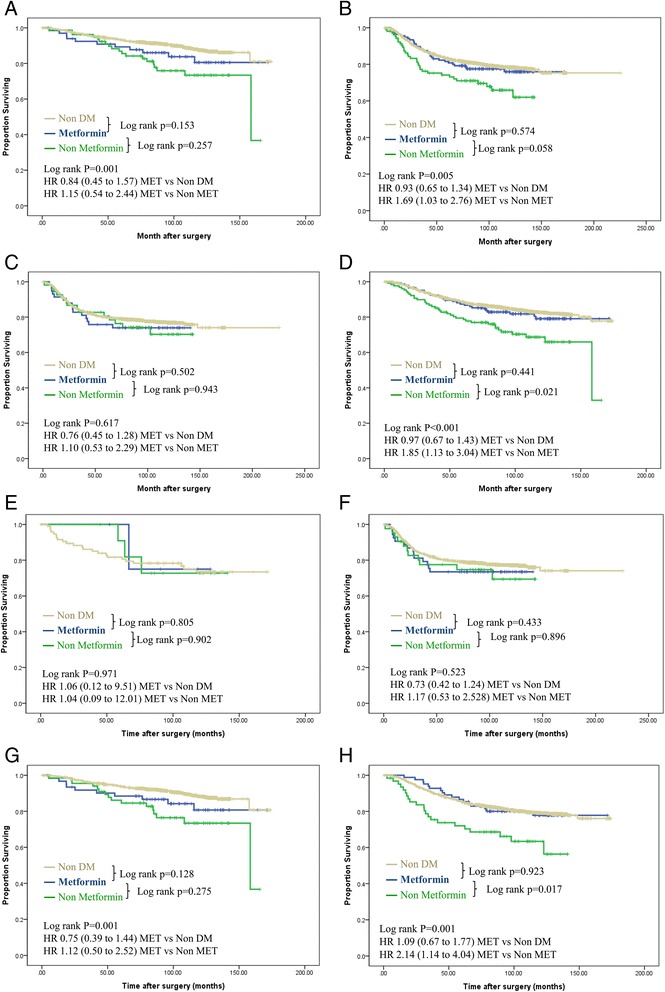
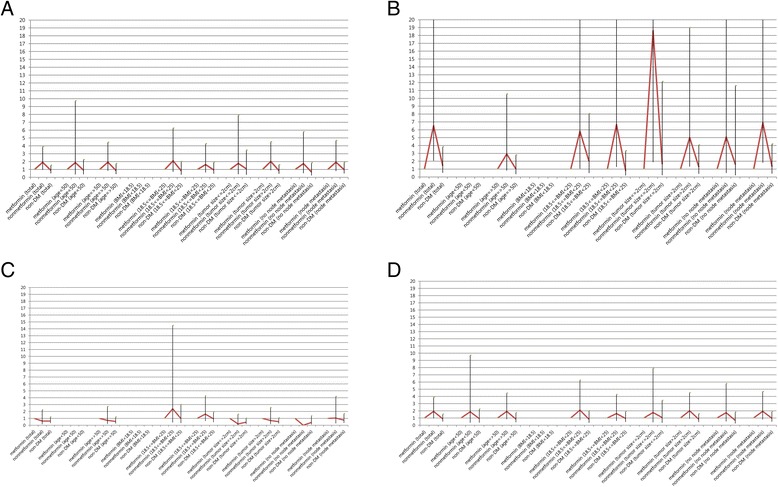
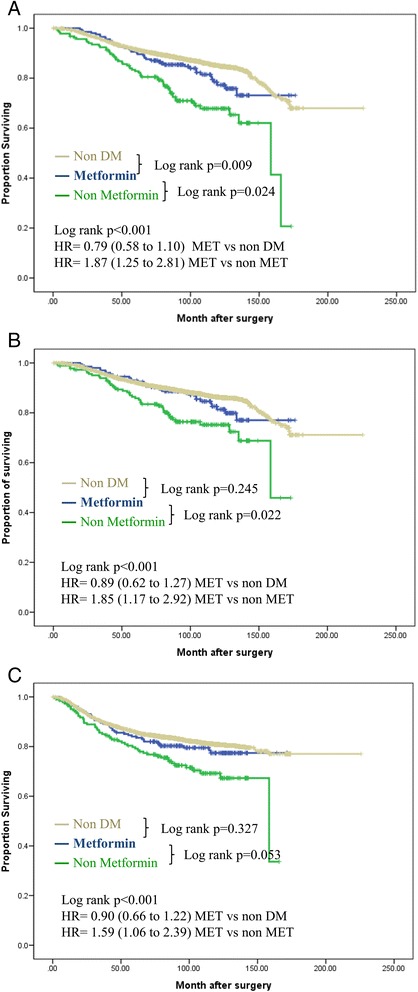
Results: In Kaplan-Meier analysis, the metformin group had a significantly better overall and cancer specific survival outcome compared with non metformin diabetic group (P <0.005 for both). There was no difference in survival between the nondiabetic and metformin groups. In multivariate analysis, Compared with metformin group, patients who did not receive metformin tended to have a higher risk of metastasis with HR 5.37 (95 % CI, 1.88 to 15.28) and breast cancer death with HR 6.51 (95 % CI, 1.88 to 15.28) on the hormone receptor-positive and HER2-negative breast cancer. The significant survival benefit of metformin observed in diabetic patients who received chemotherapy and endocrine therapy (HR for disease free survival 2.14; 95 % CI 1.14 to 4.04) was not seen in diabetic patients who did not receive these treatments.
Conclusion: Patients receiving metformin treatment when breast cancer diagnosis show a better prognosis only if they have hormone receptor-positive, HER2-positive tumors. Metformin treatment might provide a survival benefit when added to systemic therapy in diabetic patients.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
