

Cause of Death in Patients With Diabetic CKD Enrolled in the Trial to Reduce Cardiovascular Events With Aranesp Therapy (TREAT)
- PMID: 25935581
- PMCID: PMC4549188
- DOI: 10.1053/j.ajkd.2015.02.324
Cause of Death in Patients With Diabetic CKD Enrolled in the Trial to Reduce Cardiovascular Events With Aranesp Therapy (TREAT)
Abstract
Background: The cause of death in patients with chronic kidney disease (CKD) varies with CKD severity, but variation has not been quantified.
Study design: Retrospective analysis of prospective randomized clinical trial.
Setting & participants: We analyzed 4,038 individuals with anemia and diabetic CKD from TREAT, a randomized trial comparing darbepoetin alfa and placebo.
Predictors: Baseline estimated glomerular filtration rate (eGFR) and protein-creatinine ratio (PCR).
Outcomes: Cause of death as adjudicated by a blinded committee.
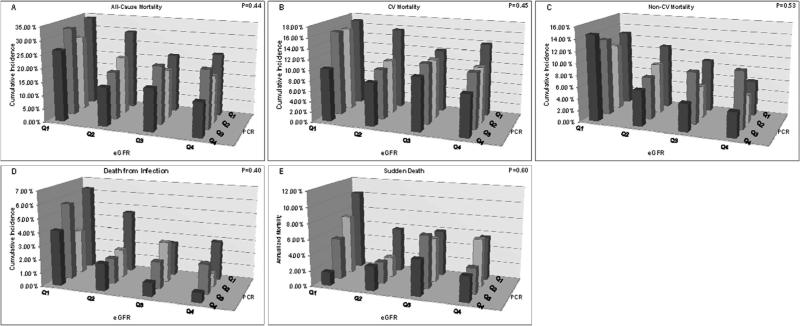
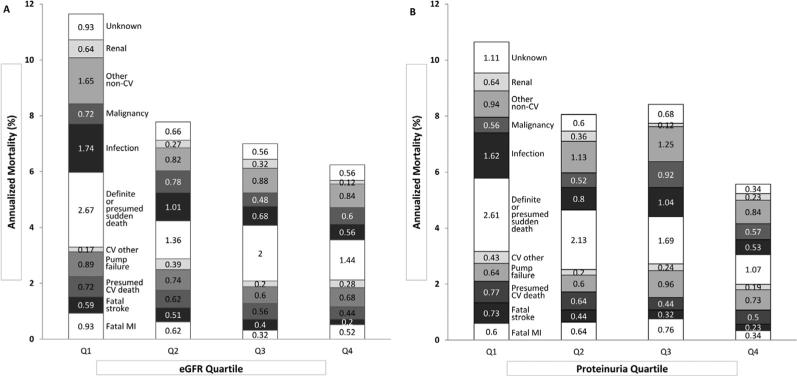
Results: Median eGFR and PCR ranged from 20.6 mL/min/1.73 m(2) and 4.1 g/g in quartile 1 (Q1) to 47.0 mL/min/1.73 m(2) and 0.1 g/g in Q4 (P<0.01). Of 806 deaths, 441, 298, and 67 were due to cardiovascular (CV), non-CV, and unknown causes, respectively. Cumulative CV mortality at 3 years was higher with lower eGFR (Q1, 15.5%; Q2, 11.1%; Q3, 11.2%; Q4, 10.3%; P<0.001) or higher PCR (Q1, 15.2%; Q2, 12.3%; Q3, 11.7%; Q4, 9.0%; P<0.001). Similarly, non-CV mortality was higher with lower eGFR (Q1, 12.7%; Q2, 8.4%; Q3, 6.7%; Q4, 6.1%; P<0.001) or higher PCR (Q1, 10.3%; Q2, 7.9%; Q3, 9.4%; Q4, 6.4%; P=0.01). Sudden death was 1.7-fold higher with lower eGFR (P=0.04) and 2.1-fold higher with higher PCR (P<0.001). Infection-related mortality was 3.3-fold higher in the lowest eGFR quartile (P<0.001) and 2.8-fold higher in the highest PCR quartile (P<0.02). The overall proportion of CV and non-CV deaths was not significantly different across eGFR or PCR quartiles.
Limitations: Results may not be generalizable to nondiabetic CKD or diabetic CKD in the absence of anemia. Measured GFR was not available.
Conclusions: In diabetic CKD, both lower baseline GFR and higher PCR are associated with higher CV and non-CV mortality rates, particularly from sudden death and infection. Efforts to improve outcomes should focus on CV disease and early diagnosis and treatment of infection.
Keywords: Chronic kidney disease (CKD); Trial to Reduce Cardiovascular Events With Aranesp Therapy (TREAT); anemia; cardiovascular (CV) disease; diabetic CKD; estimated glomerular filtration rate (eGFR); infection; mortality; protein-creatinine ratio (PCR); proteinuria; renal function; sudden death.
Copyright © 2015 National Kidney Foundation, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–1305. - PubMed
-
- Anavekar NS, McMurray JJ, Velazquez EJ, et al. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med. 2004;351:1285–1295. - PubMed
-
- Clase CM, Gao P, Tobe SW, et al. Estimated glomerular filtration rate and albuminuria as predictors of outcomes in patients with high cardiovascular risk: a cohort study. Ann Intern Med. 2011;154:310–318. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
