

A Randomized Clinical Trial of Jet-Injected Lidocaine to Reduce Venipuncture Pain for Young Children
- PMID: 25935844
- PMCID: PMC4863077
- DOI: 10.1016/j.annemergmed.2015.04.003
A Randomized Clinical Trial of Jet-Injected Lidocaine to Reduce Venipuncture Pain for Young Children
Abstract
Study objective: The J-Tip (National Medical Products Inc, Irvine, CA) uses air instead of a needle to push lidocaine into the skin. To our knowledge, no studies have investigated its use for venipuncture in young children. We determine whether the J-Tip decreased venipuncture pain in young children compared with vapocoolant spray.
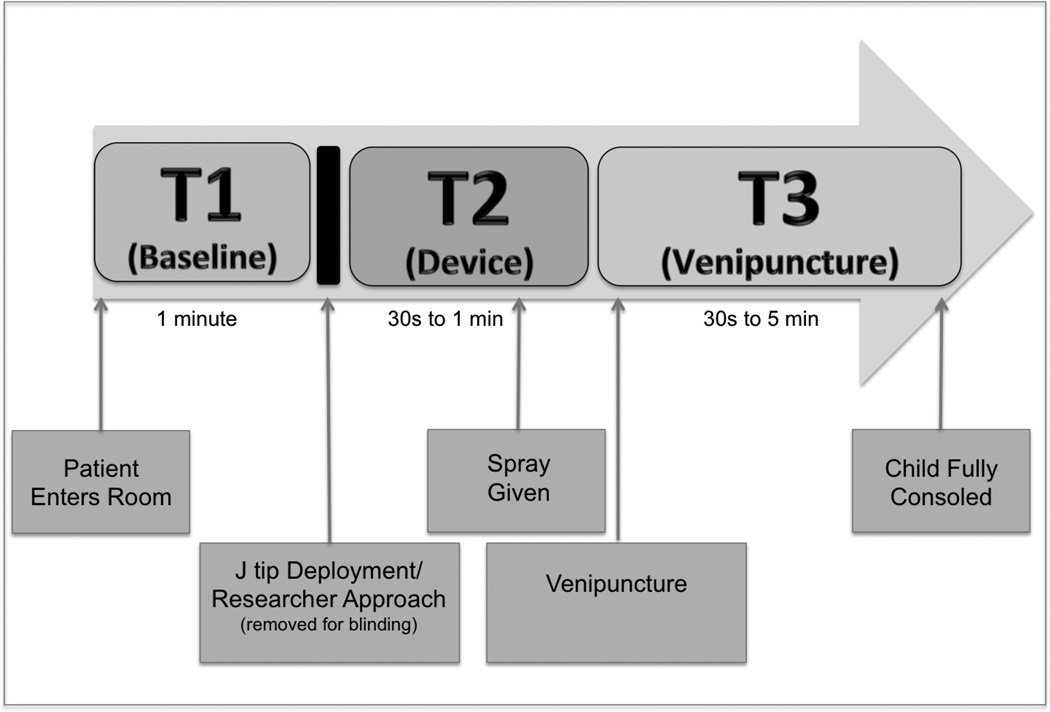
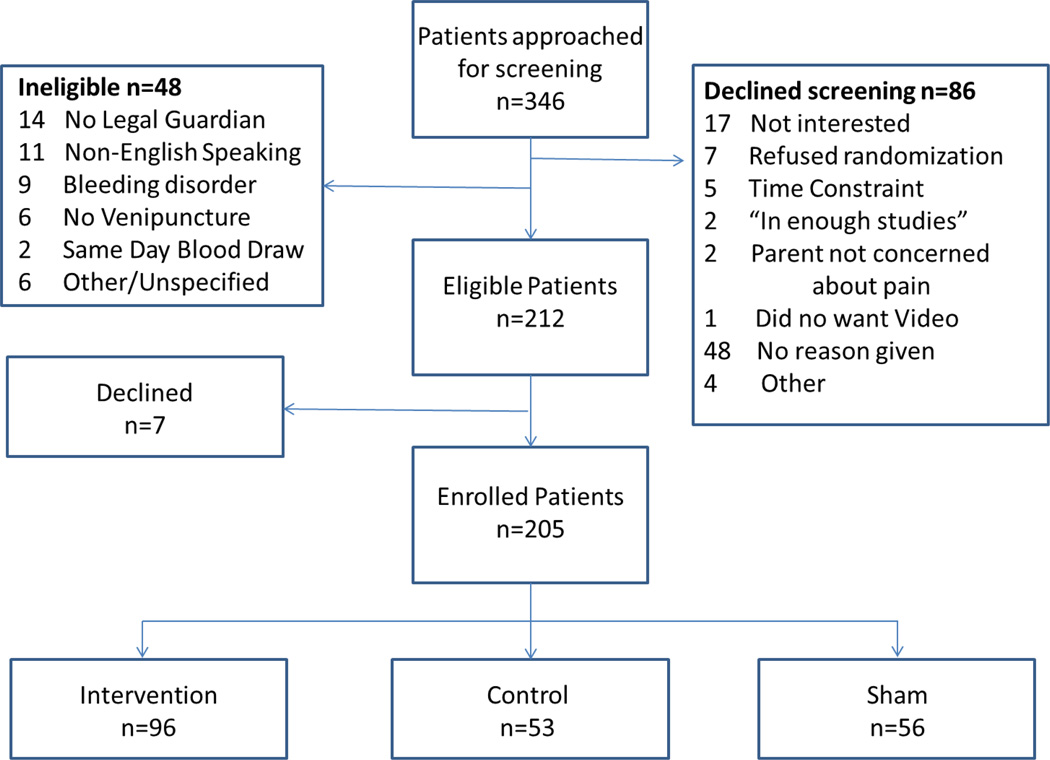
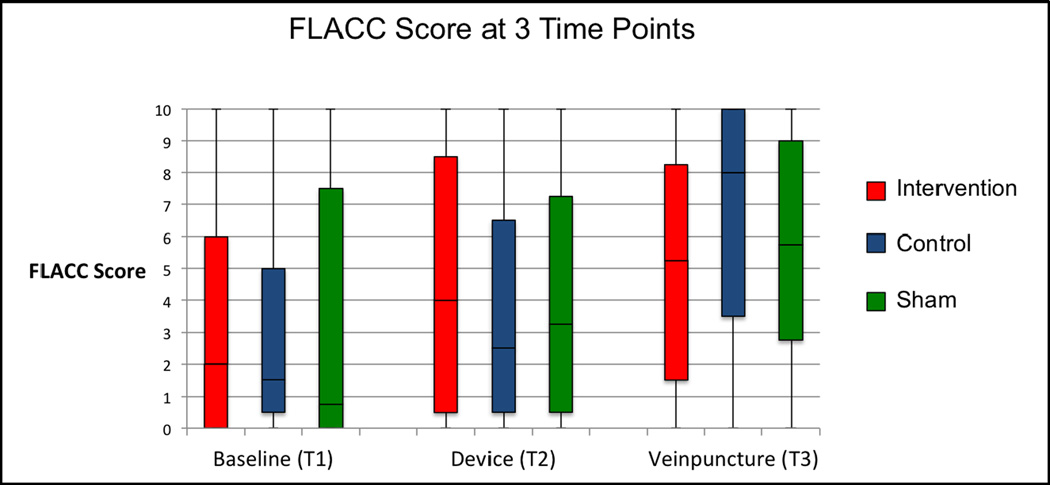
Methods: Children aged 1 to 6 years were randomized into 3 groups: intervention (J-Tip), control (vapocoolant spray), and sham (vapocoolant spray and pop of an empty J-Tip). The procedure was videotaped and scored with the Face, Legs, Activity, Cry and Consolability (FLACC) tool at 3 points; baseline, before approach; device, at J-Tip deployment; and at venipuncture. The FLACC tool was scored 0 (none) to 10 (severe). Comparisons of pain scores over time were made with the generalized estimating equation. Venipuncture success and adverse effects were assessed and compared with χ(2).
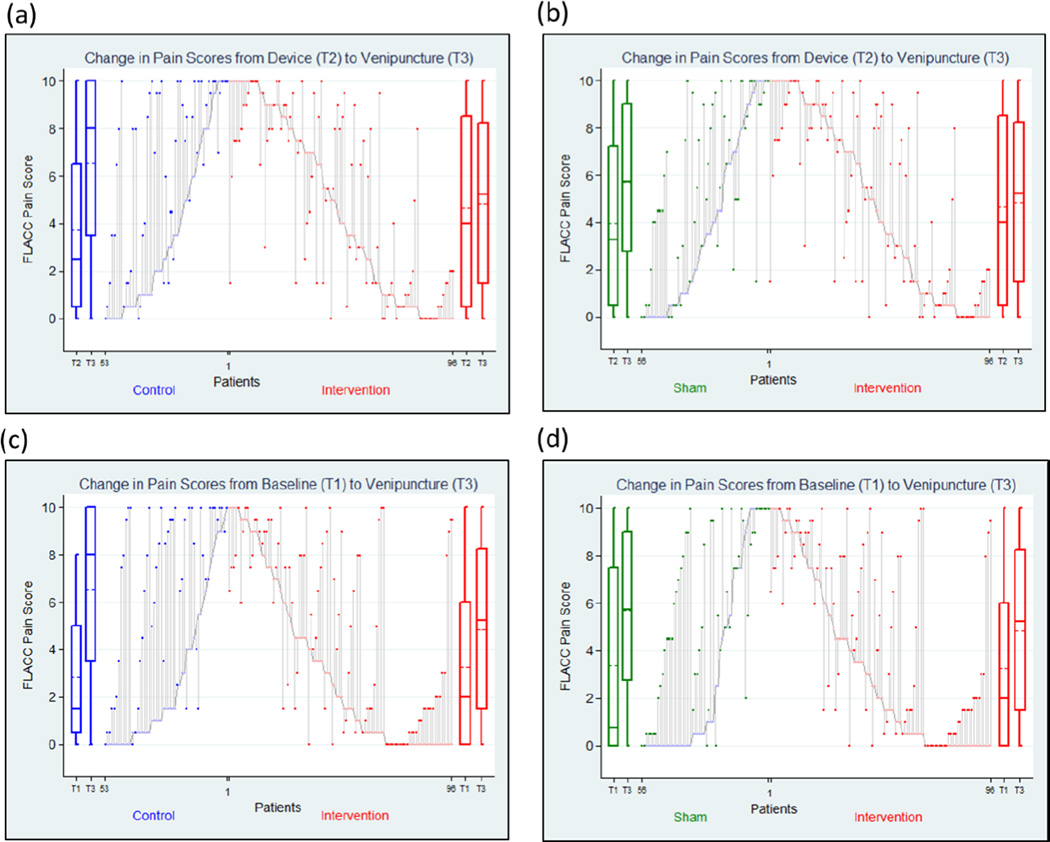
Results: Two hundred five children enrolled: intervention 96, control 53, and sham 56. There were no between-group differences in baseline characteristics. There was no mean change in pain scores from device to venipuncture in the intervention group (0.26; 95% confidence interval [CI] -0.31 to 0.82), but there was an increase in pain in the control (2.82; 95% CI 1.91 to 3.74) and sham (1.68; 95% CI 0.83 to 2.52) groups. This change was greater for the control and sham compared to the intervention group. There was no difference in venipuncture success between groups. No severe adverse events occurred. Minor adverse events were the same between groups.
Conclusion: Use of the J-Tip for children aged 1 to 6 years reduced venipuncture pain compared with vapocoolant spray or sham treatment.
Copyright © 2015 American College of Emergency Physicians. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures

References
-
- Cohen LL. Behavioral Approaches to Anxiety and Pain Management for Pediatric Venous Access. Pediatrics. 2008;112:S134–S139. - PubMed
-
- Weisman SJ, Bernstein B, Schechter NL. Consequences of Inadequate Analgesia During Painful Procedures in Children. Arch Pediatr Adolesc Med. 1998;152:147–149. - PubMed
-
- Fradet C, McGrath PJ, Kay J, Adams S, Luke B. A prospective survey of reactions to blood tests by children and adolescents. Pain. 1990;40:53–60. - PubMed
-
- American Academy of Pediatrics, Committee on Psychosocial Aspects of Child and Family Health; American Pain Society Task Force on Pain in Infants, Children and Adolescents. The assessment and management of acute pain in infants, children and adolescents. Pediatrics. 2001:793–797.
-
- Spanos S, Booth R, Koenig H, Sikes K, Gracely E, Kim IK. Jet Injection of 1% Buffered Lidocaine versus Topical ELA-Max for Anesthesia Before Peripheral Intravenous Catheterization in Children. Pediatr Emerg Care. 2008;24:511–515. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
