

Gallbladder perforation and massive intra-abdominal haemorrhage complicating acute cholecystitis in a patient with haemophilia A
- PMID: 25935908
- PMCID: PMC4434330
- DOI: 10.1136/bcr-2014-205971
Gallbladder perforation and massive intra-abdominal haemorrhage complicating acute cholecystitis in a patient with haemophilia A
Abstract
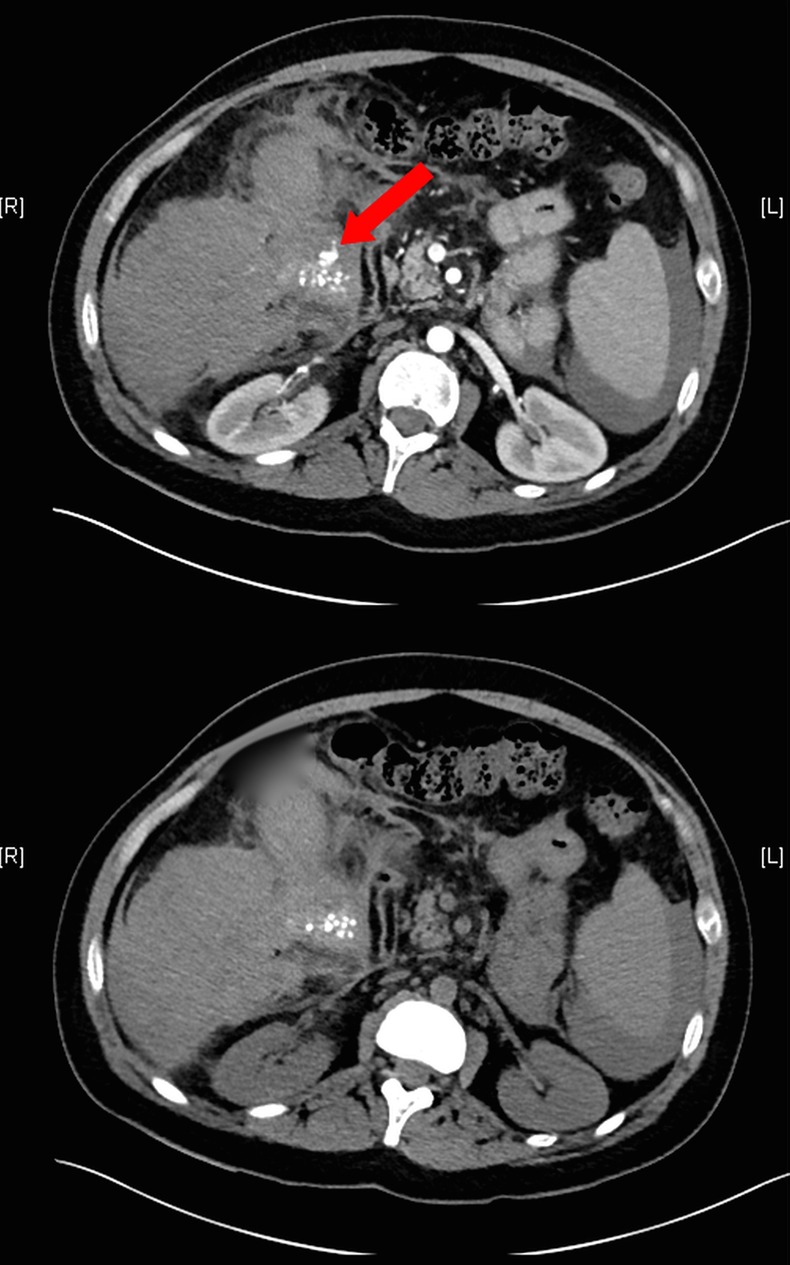
We present an unusual case of a 32-year-old man with haemophilia A, who sustained massive, haemodynamically significant intra-abdominal bleeding from a perforated gallbladder wall and from the greater omentum as a complication of acute ulcerophlegmonous and haemorrhagic cholecystitis. Recombinant coagulation factor VIII was given and an emergency laparotomy was performed, with open cholecystectomy and haemostasis. Coagulation factor VIII was given for a further 2 weeks postoperatively, and the patient was discharged in good condition. In most published cases of haemorrhagic cholecystitis, the haemoperitoneum arises via transhepatic perforation; in this case, there was a free rupture into the peritoneal cavity. Patients with coagulopathies may have severe haemorrhagic complications and therefore need interdisciplinary management before, during and after surgery. Replacement therapy with factor concentrates should be initiated at once, and early surgery for gallbladder disease should be considered.
2015 BMJ Publishing Group Ltd.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical