

Propranolol attenuates hemorrhage and accelerates wound healing in severely burned adults
- PMID: 25936635
- PMCID: PMC4432824
- DOI: 10.1186/s13054-015-0913-x
Propranolol attenuates hemorrhage and accelerates wound healing in severely burned adults
Abstract
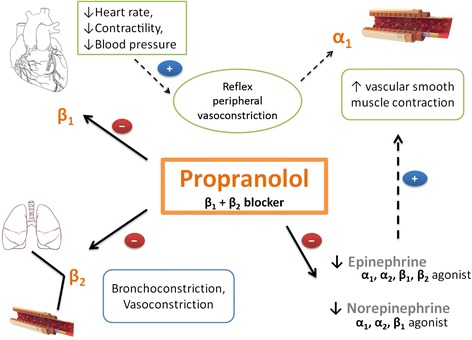
Introduction: Propranolol, a nonselective β-blocker, exerts an indirect effect on the vasculature by leaving α-adrenergic receptors unopposed, resulting in peripheral vasoconstriction. We have previously shown that propranolol diminishes peripheral blood following burn injury by increasing vascular resistance. The purpose of this study was to investigate whether wound healing and perioperative hemodynamics are affected by propranolol administration in severely burned adults.
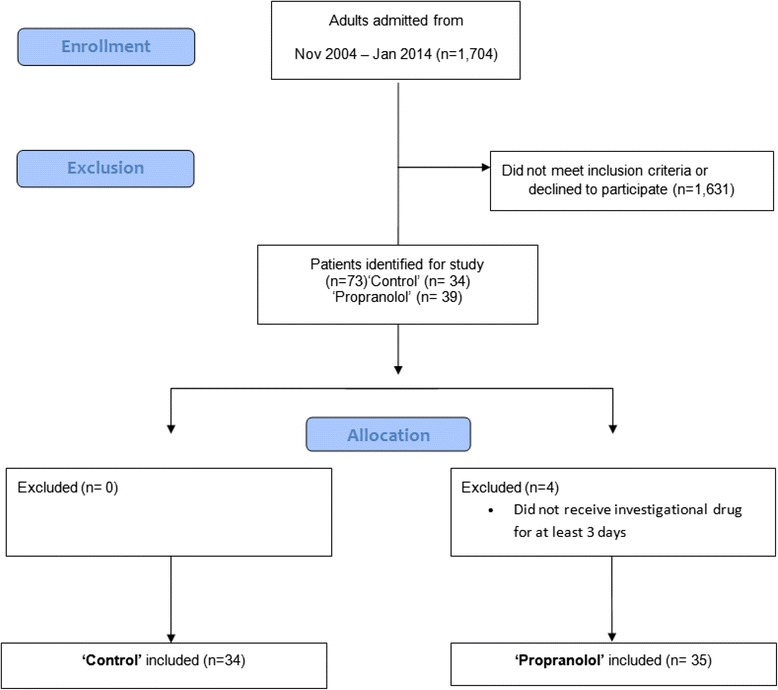
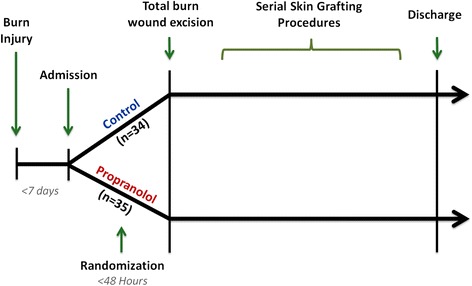
Methods: Sixty-nine adult patients with burns covering ≥ 30% of the total body surface area (TBSA) were enrolled in this IRB-approved study. Patients received standard burn care with (n = 35) or without (control, n = 34) propranolol. Propranolol was administered within 48 hours of burns and given throughout hospital discharge to decrease heart rate by approximately 20% from admission levels. Wound healing was determined by comparing the time between grafting procedures. Blood loss was determined by comparing pre- and postoperative hematocrit while factoring in operative graft area. Data were collected between first admission and first discharge.
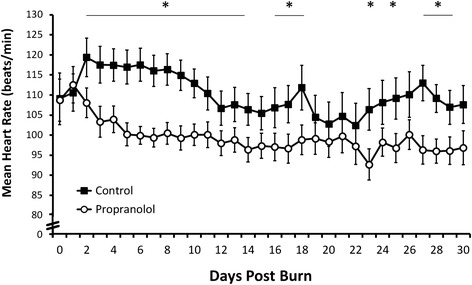
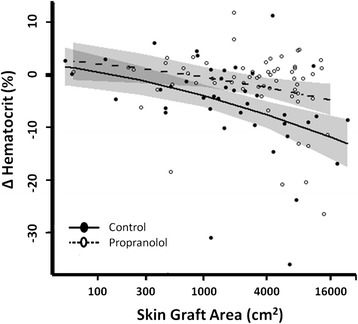
Results: Demographics, burn size, and mortality were comparable in the control and propranolol groups. Patients in the propranolol group received an average propranolol dose of 3.3 ± 3.0 mg/kg/day. Daily average heart rate over the first 30 days was significantly lower in the propranolol group (P < 0.05). The average number of days between skin grafting procedures was also lower in propranolol patients (10 ± 5 days) than in control patients (17 ± 12 days; P = 0.02), indicative of a faster donor site healing time in the propranolol group. Packed red blood cell infusion was similar between groups (control 5.3 ± 5.4 units vs. propranolol 4.4 ± 3.1 units, P = 0.89). Propranolol was associated with a 5 to 7% improvement in perioperative hematocrit during grafting procedures of 4,000 to 16,000 cm(2) compared to control (P = 0.002).
Conclusions: Administration of propranolol during the acute hospitalization period diminishes blood loss during skin grafting procedures and markedly improves wound healing in severely burned adults. As burn patients require serial surgical interventions for motor and cosmetic repair, restricting blood loss during operative intervention is optimal.
Figures
References
-
- Wilmore DW, Aulick LH. Metabolic changes in burned patients. Surg Clin North Am. 1978;58:1173–1187. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01-112936-01/PHS HHS/United States
- R01-GM056687/GM/NIGMS NIH HHS/United States
- R01 HD049471/HD/NICHD NIH HHS/United States
- P50-GM060338/GM/NIGMS NIH HHS/United States
- R01 GM112936/GM/NIGMS NIH HHS/United States
- UL1TR000071/TR/NCATS NIH HHS/United States
- UL1 TR000071/TR/NCATS NIH HHS/United States
- T32-GM008256/GM/NIGMS NIH HHS/United States
- R01 GM056687/GM/NIGMS NIH HHS/United States
- P50 GM060338/GM/NIGMS NIH HHS/United States
- T32 GM008256/GM/NIGMS NIH HHS/United States
- R01-HD049471/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
