

Neuroimaging-Aided Prediction of the Effect of Methylphenidate in Children with Attention-Deficit Hyperactivity Disorder: A Randomized Controlled Trial
- PMID: 25936640
- PMCID: PMC4864654
- DOI: 10.1038/npp.2015.128
Neuroimaging-Aided Prediction of the Effect of Methylphenidate in Children with Attention-Deficit Hyperactivity Disorder: A Randomized Controlled Trial
Erratum in
-
Neuroimaging-Aided Prediction of the Effect of Methylphenidate in Children with Attention-Deficit Hyperactivity Disorder: A Randomized Controlled Trial.Neuropsychopharmacology. 2015 Nov;40(12):2852. doi: 10.1038/npp.2015.154. Epub 2015 Jul 8. Neuropsychopharmacology. 2015. PMID: 26152808 Free PMC article. No abstract available.
Abstract
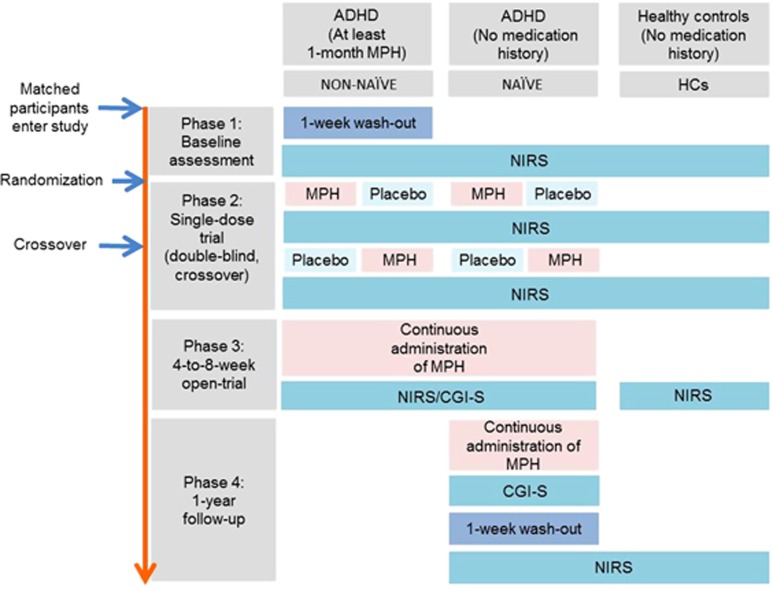
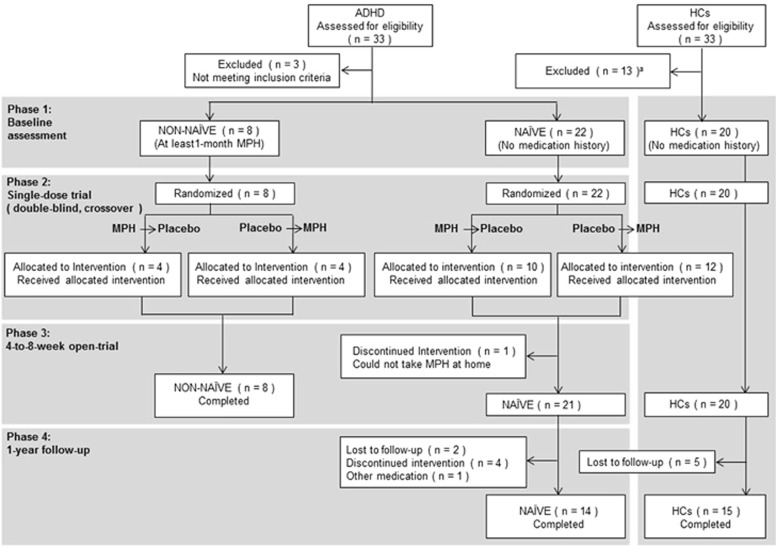
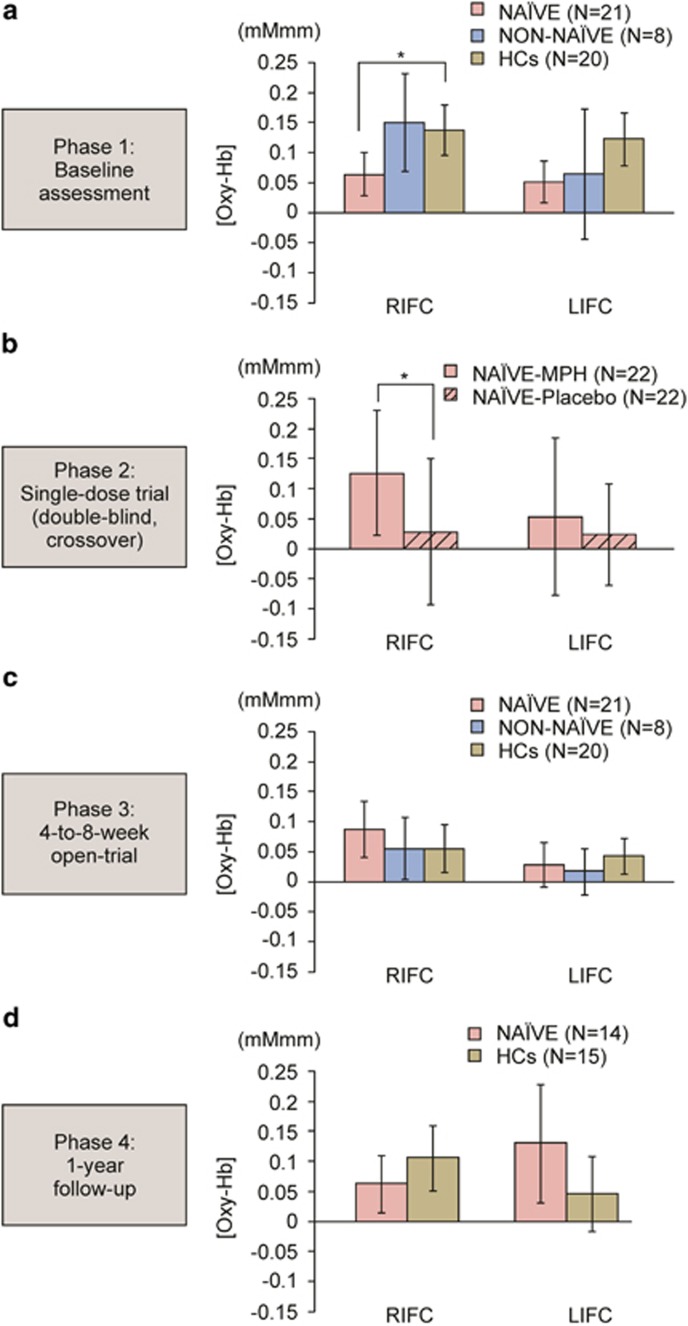
Although methylphenidate hydrochloride (MPH) is a first-line treatment for children with attention-deficit hyperactivity disorder (ADHD), the non-response rate is 30%. Our aim was to develop a supplementary neuroimaging biomarker for predicting the clinical effect of continuous MPH administration by using near-infrared spectroscopy (NIRS). After baseline assessment, we performed a double-blind, placebo-controlled, crossover trial with a single dose of MPH, followed by a prospective 4-to-8-week open trial with continuous MPH administration, and an ancillary 1-year follow-up. Twenty-two drug-naïve and eight previously treated children with ADHD (NAÏVE and NON-NAÏVE) were compared with 20 healthy controls (HCs) who underwent multiple NIRS measurements without intervention. We tested whether NIRS signals at the baseline assessment or ΔNIRS (single dose of MPH minus baseline assessment) predict the Clinical Global Impressions-Severity (CGI-S) score after 4-to-8-week or 1-year MPH administration. The secondary outcomes were the effect of MPH on NIRS signals after single-dose, 4-to-8-week, and 1-year administration. ΔNIRS significantly predicted CGI-S after 4-to-8-week MPH administration. The leave-one-out classification algorithm had 81% accuracy using the NIRS signal. ΔNIRS also significantly predicted CGI-S scores after 1 year of MPH administration. For secondary analyses, NAÏVE exhibited significantly lower prefrontal activation than HCs at the baseline assessment, whereas NON-NAÏVE and HCs showed similar activation. A single dose of MPH significantly increased activation compared with the placebo in NAÏVE. After 4-to-8-week administration, and even after MPH washout following 1-year administration, NAÏVE demonstrated normalized prefrontal activation. Supplementary NIRS measurements may serve as an objective biomarker for clinical decisions and monitoring concerning continuous MPH treatment in children with ADHD.
Figures

References
-
- Achenbach TM, Howell CT, Quay HC, Conners CK (1991). National survey of problems and competencies among four- to sixteen-year-olds: parents' reports for normative and clinical samples. Monogr Soc Res Child Dev 56: 1–131. - PubMed
-
- Borgwardt S, Fusar-Poli P (2012). Third-generation neuroimaging in early schizophrenia: translating research evidence into clinical utility. Br J Psychiatry 200: 270–272. - PubMed
-
- Buitelaar JK, Van der Gaag RJ, Swaab-Barneveld H, Kuiper M (1995). Prediction of clinical response to methylphenidate in children with attention-deficit hyperactivity disorder. J Am Acad Child Adolesc Psychiatry 34: 1025–1032. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
