

Dosimetric Predictors of Radiation-Induced Vaginal Stenosis After Pelvic Radiation Therapy for Rectal and Anal Cancer
- PMID: 25936810
- PMCID: PMC4822494
- DOI: 10.1016/j.ijrobp.2015.02.029
Dosimetric Predictors of Radiation-Induced Vaginal Stenosis After Pelvic Radiation Therapy for Rectal and Anal Cancer
Abstract
Purpose: Although vaginal stenosis (VS) is a recognized toxicity in women who receive pelvic radiation therapy (RT), the relationship between RT dose and the volume and extent of toxicity has not been analyzed. We modeled this relationship to identify predictors of VS.
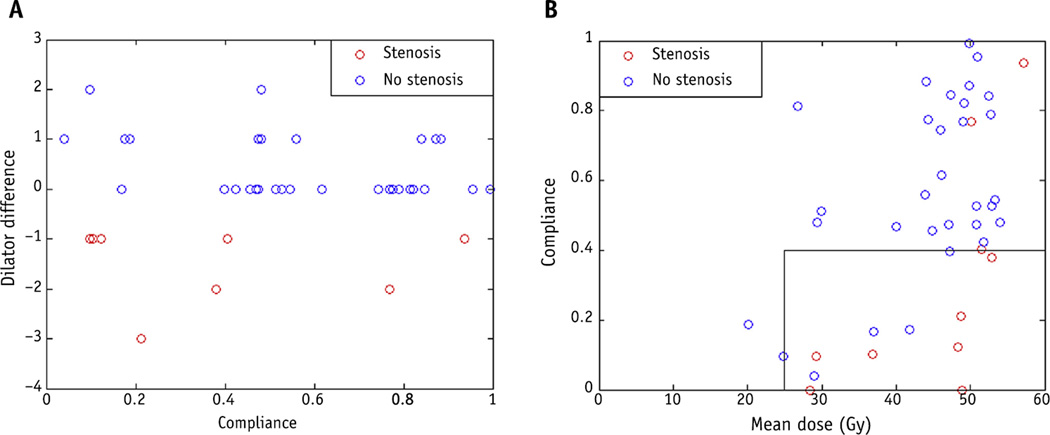
Methods and materials: We evaluated 54 women, aged 29 to 78 years, who underwent pelvic RT for rectal or anal cancer during 2008 to 2011 and were enrolled in a prospective study evaluating vaginal dilator use. Maximum dilator size was measured before RT (baseline) and 1 month and 12 months after RT. Dilator use was initiated at 1 month. The difference (D) in dilator size before and after RT was recorded. Those with D ≤-1 were classified as having VS (n=35); those with D ≥0 were classified as having no VS (n=19 at 1 month). Dose-volume parameters were extracted, and the generalized equivalent uniform dose (gEUD) was used to build a predictive model.
Results: The mean vaginal doses were 50.0 Gy and 36.8 Gy for anal and rectal cancer patients, respectively. One month after RT, a gEUD model using a wide range of a values suggests that sparing of vaginal volume to a low dose may be important. When gEUD (a = -1) was <35 Gy and the mean vaginal dose was <43 Gy, severe VS was reduced (P=.02). A 1-year analysis suggests increasingly negative D values with increasing mean dose. However, patients with compliance <40% were more likely to have toxicity.
Conclusions: Vaginal stenosis is influenced by multiple RT dose-volume characteristics. Mean dose and gEUD constraints together may reduce the risk of severe VS. Patients receiving higher mean vaginal doses should have greater compliance with dilator therapy to minimize risk of toxicity. Further validation with independent datasets is needed.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: none.
Figures




References
-
- Grigsby PW, Russell A, Bruner D, et al. Late injury of cancer therapy on the female reproductive tract. Int J Radiat Oncol Biol Phys. 1995;31:1281–1299. - PubMed
-
- Mirabeau-Beale KL, Viswanathan AN. Quality of life (QOL) in women treated for gynecologic malignancies with RT: A literature review of patient-reported outcomes. Gynecol Oncol. 2014;134:403–409. - PubMed
-
- Bergmark K, Avall-Lundqvist E, Dickman PW, et al. Vaginal changes and sexuality in women with a history of cervical cancer. N Engl J Med. 1999;340:1383–1389. - PubMed
-
- Brand AH, Bull CA, Cakir B. Vaginal stenosis in patients treated with radiotherapy for carcinoma of the cervix. Int J Gynecol Cancer. 2006;16:288–293. - PubMed
-
- Bruner DW, Lanciano R, Keegan M, et al. Vaginal stenosis and sexual function following intracavitary radiation for the treatment of cervical and endometrial carcinoma. Int J Radiat Oncol Biol Phys. 1993;27:825–830. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
