

4Ps medicine of the fatty liver: the research model of predictive, preventive, personalized and participatory medicine-recommendations for facing obesity, fatty liver and fibrosis epidemics
- PMID: 25937854
- PMCID: PMC4417534
- DOI: 10.1186/1878-5085-5-21
4Ps medicine of the fatty liver: the research model of predictive, preventive, personalized and participatory medicine-recommendations for facing obesity, fatty liver and fibrosis epidemics
Abstract
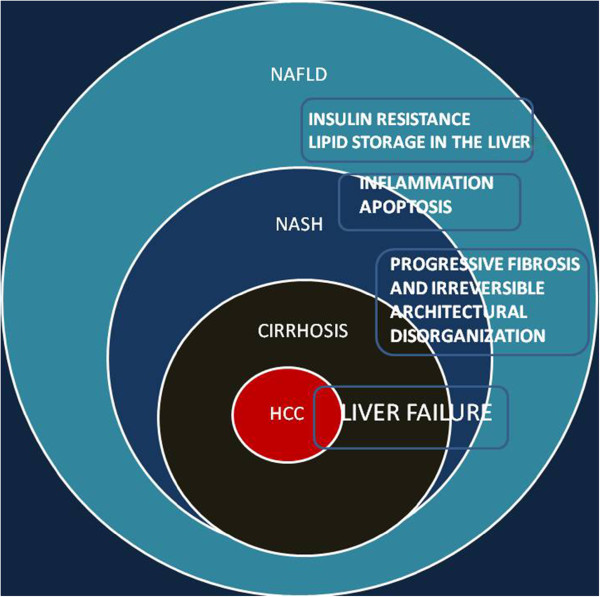
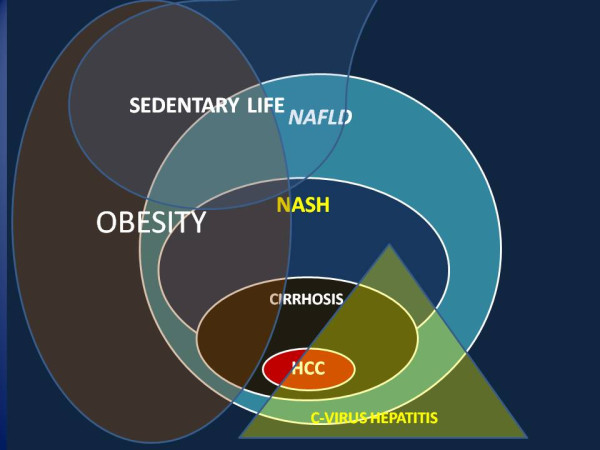
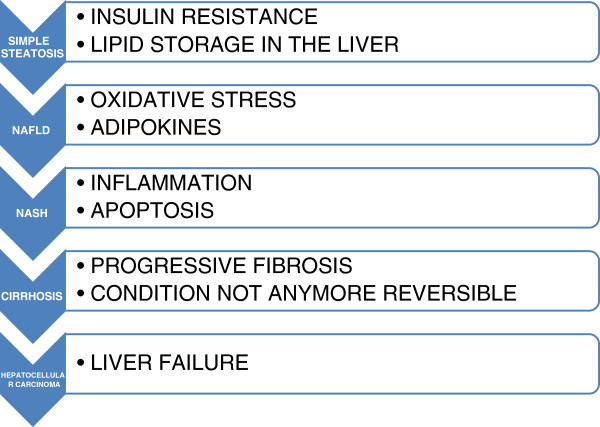
Relationship between adipose tissue and fatty liver, and its possible evolution in fibrosis, is supported by clinical and research experience. Given the multifactorial pathogenesis of non-alcoholic fatty liver disease (NAFLD), treatments for various contributory risk factors have been proposed; however, there is no single validated therapy or drug association recommended for all cases which can stand alone. Mechanisms, diagnostics, prevention and treatment of obesity, fatty liver and insulin resistance are displayed along with recommendations and position points. Evidences and practice can get sustainable and cost-benefit valuable outcomes by participatory interventions. These recommendations can be enhanced by comprehensive research projects, addressed to societal issues and innovation, market appeal and industry development, cultural acceptance and sustainability. The basis of participatory medicine is a greater widespread awareness of a condition which is both a disease and an easy documented and inclusive clue for associated diseases and unhealthy lifestyle. This model is suitable for addressing prevention and useful for monitoring improvement, worsening and adherence with non-invasive imaging tools which allow targeted approaches. The latter include health psychology and nutritional and physical exercise prescription expertise disseminated by continuous medical education but, more important, by concrete curricula for training undergraduate and postgraduate students. It is possible and recommended to do it by early formal teaching of ultrasound imaging procedures and of practical lifestyle intervention strategies, including approaches aimed to healthier fashion suggestions. Guidelines and requirements of research project funding calls should be addressed also to NAFLD and allied conditions and should encompass the goal of training by research and the inclusion of participatory medicine topics. A deeper awareness of ethics of competences in health professionals and the articulation of knowledge, expertise and skills of medical doctors, dieticians, health psychologists and sport and physical exercise graduates are the necessary strategy for detectin a suboptimal health status and achieving realistically beneficial lifestyle changes. "The devil has put a penalty on all things we enjoy in life. Either we suffer in health or we suffer in soul or we get fat" (Albert Einstein); the task of medical research and intervention is to make possible to enjoy life also without things that make sufferance in health and souls and which excessively increase body fat.
Keywords: Adipose tissue; Diet; Fashion; Fatty liver; Interactome; Lifestyle; Liver fibrosis; Obesity; Suboptimal Health.
Figures
References
-
- Cinti S. Between brown and white: novel aspects of adipocyte differentiation. Ann Med. 2011;43(2):104–115. - PubMed
-
- Ukkola O, Santaniemi M. Adiponectin: a link between excess adiposity and associated comorbidities? J Mol Med (Berl) 2002;80(11):696–702. - PubMed
-
- Koehler EM, Schouten JN, Hansen BE, van Rooij FJ, Hofman A, Stricker BH, Janssen HL. Prevalence and risk factors of non-alcoholic fatty liver disease in the elderly: results from the Rotterdam Study. J Hepatol. 2012;57(6):1305–1311. - PubMed
-
- Milić S, Stimac D. Nonalcoholic fatty liver disease/steatohepatitis: epidemiology, pathogenesis, clinical presentation and treatment. Dig Dis. 2012;30(2):158–162. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
