

Costs to Health Services and the Patient of Treating Tuberculosis: A Systematic Literature Review
- PMID: 25939501
- PMCID: PMC4559093
- DOI: 10.1007/s40273-015-0279-6
Costs to Health Services and the Patient of Treating Tuberculosis: A Systematic Literature Review
Abstract
Background: Novel tuberculosis (TB) drugs and the need to treat drug-resistant tuberculosis (DR-TB) are likely to bring about substantial transformations in TB treatment in coming years. An evidence base for cost and cost-effectiveness analyses of these developments is needed.
Objective: Our objective was to perform a review of papers assessing provider-incurred as well as patient-incurred costs of treating both drug-susceptible (DS) and multidrug-resistant (MDR)-TB.
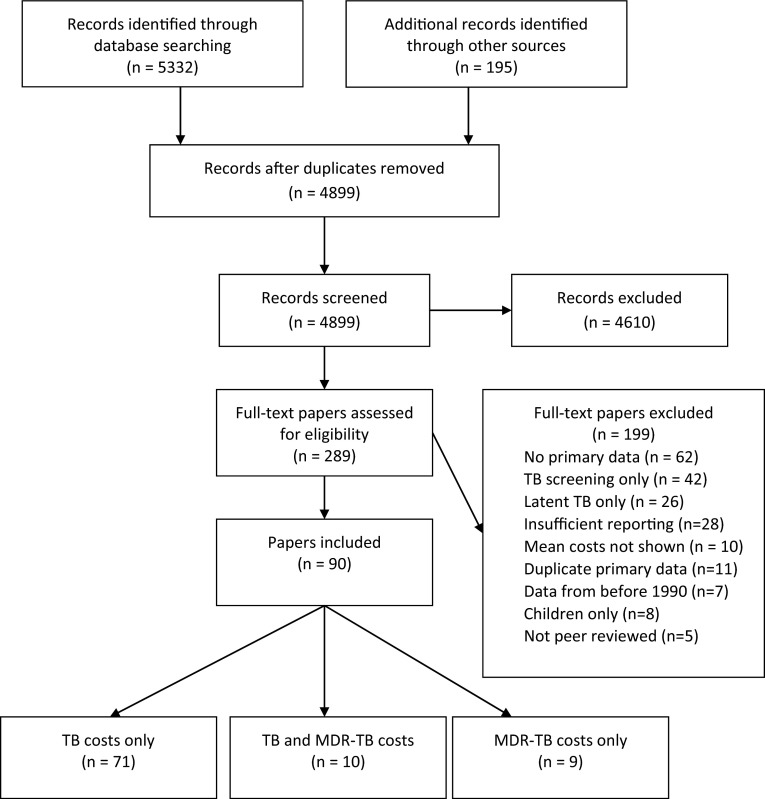
Methods: Five databases (EMBASE, Medline, the National Health Service Economic Evaluation Database, the Cost-Effectiveness Analysis Registry, and Latin American and Caribbean Health Services Literature) were searched for cost and economic evaluation full-text papers containing primary DS-TB and MDR-TB treatment cost data published in peer-reviewed journals between January 1990 and February 2015. No language restrictions were set. The search terms were a combination of 'tuberculosis', 'multidrug-resistant tuberculosis', 'cost', and 'treatment'. In the selected papers, study methods and characteristics, quality indicators and costs were extracted into summary tables according to pre-defined criteria. Results were analysed according to country income groups and for provider costs, patient costs and productivity losses. All values were converted to $US, year 2014 values, so that studies could be compared.
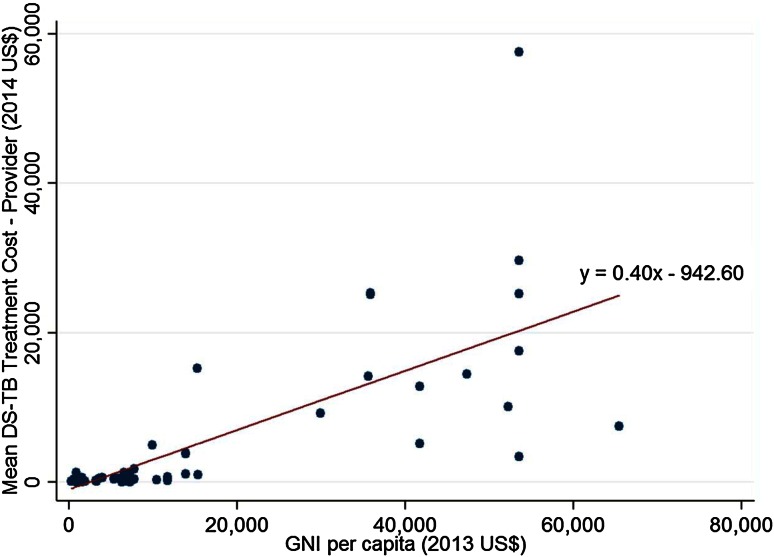
Results: We selected 71 treatment cost papers on DS-TB only, ten papers on MDR-TB only and nine papers that included both DS-TB and MDR-TB. These papers provided evidence on the costs of treating DS-TB and MDR-TB in 50 and 16 countries, respectively. In 31 % of the papers, only provider costs were included; 26 % included only patient-incurred costs, and the remaining 43 % estimated costs incurred by both. From the provider perspective, mean DS-TB treatment costs per patient were US$14,659 in high-income countries (HICs), US$840 in upper middle-income countries (UMICs), US$273 in lower middle-income (LMICs), and US$258 in low-income countries (LICs), showing a strong positive correlation. The respective costs for treating MDR-TB were US$83,365, US$5284, US$6313 and US$1218. Costs incurred by patients when seeking treatment for DS-TB accounted for an additional 3 % of the provider costs in HICs. A greater burden was seen in the other income groups, increasing the costs of DS-TB treatment by 72 % in UMICs, 60 % in LICs and 31 % in LMICs. When provider costs, patient costs and productivity losses were combined, productivity losses accounted for 16 % in HICs, 29 % in UMICs, 40 % in LMICs and 38 % in LICs.
Conclusion: Cost data for MDR-TB treatment are limited, and the variation in delivery mechanisms, as well as the rapidly evolving diagnosis and treatment regimens, means that it is essential to increase the number of studies assessing the cost from both provider and patient perspectives. There is substantial evidence available on the costs of DS-TB treatment from all regions of the world. The patient-incurred costs illustrate that the financial burden of illness is relatively greater for patients in poorer countries without universal healthcare coverage.
Figures
References
-
- WHO. The End TB Strategy: Global strategy and targets for tuberculosis prevention, care and control after 2015. In: World Health Organisation, editor. WHO Global Tuberculosis Report. Geneva: WHO; 2014. p. 23.
-
- Fryatt RJ. Review of published cost-effectiveness studies on tuberculosis treatment programmes. Int J Tuberc Lung Dis. 1997;1(2):101–109. - PubMed
-
- Russell S. The economic burden of illness for households in developing countries: a review of studies focusing on malaria, tuberculosis, and human immunodeficiency virus/acquired immunodeficiency syndrome. Am J Trop Med Hyg. 2004;71(2 Suppl):147–155. - PubMed
-
- Verdier JE, et al. A systematic review of economic evaluation studies of tuberculosis control in high-income countries. Int J Tuberc Lung Dis. 2011;15(12):1587–1598. - PubMed
-
- Ukwaja KN, et al. The economic burden of tuberculosis care for patients and households in Africa: a systematic review. Int J Tuberc Lung Dis. 2012;16(6):733–739. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
