

Laparoscopic suturing learning curve in an open versus closed box trainer
- PMID: 25939742
- PMCID: PMC4710670
- DOI: 10.1007/s00464-015-4211-0
Laparoscopic suturing learning curve in an open versus closed box trainer
Abstract
Background: The aim of this study was to examine the influence of training under direct vision prior to training with indirect vision on the learning curve of the laparoscopic suture task.
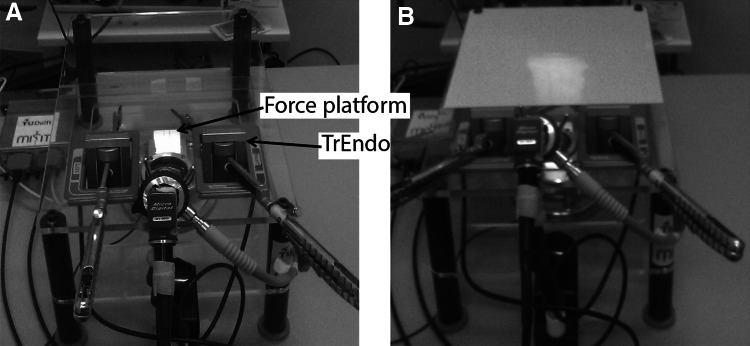
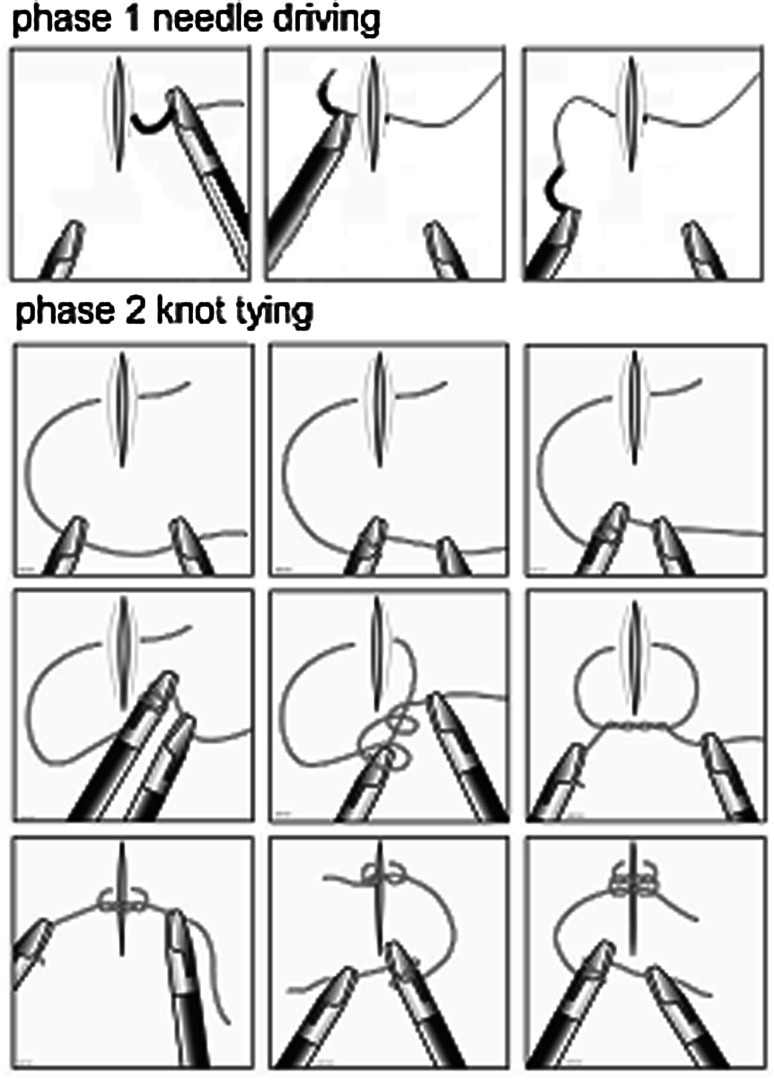
Methods: Novices were randomized in two groups. Group 1 performed three suturing tasks in a transparent laparoscopic box trainer under direct vision followed by three suturing tasks in a standard non-transparent laparoscopic box trainer equipped with a 0° laparoscope. Group 2 performed six suturing tasks in a standard laparoscopic box trainer. Performance time, motion analysis parameters (economy of movements) and interaction force parameters (tissue handling) were measured. Participants completed a questionnaire assessing: self-perceived dexterity before and after the training, their experienced frustration and the difficulty of the training.
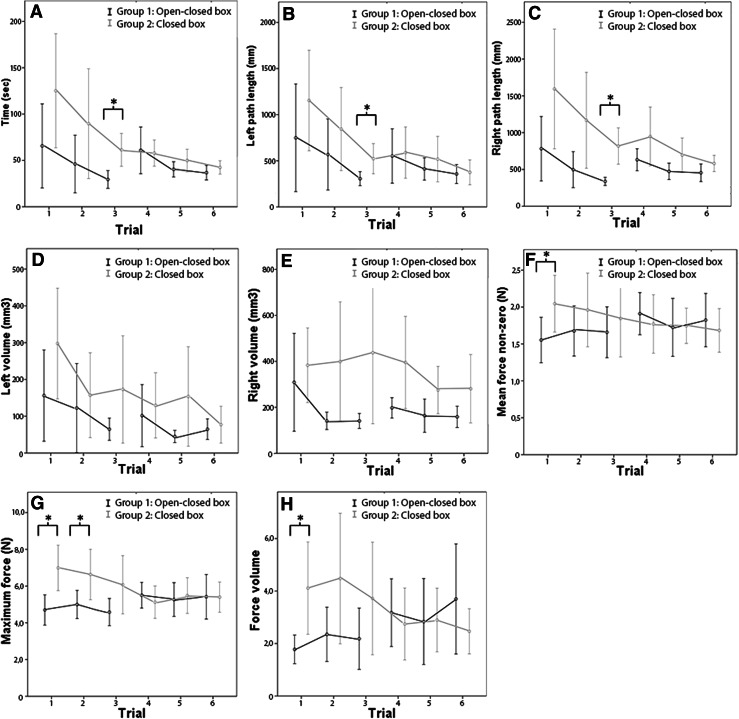
Results: A total of 34 participants were included, one was excluded because of incomplete training. Group 1 used significantly less time to complete the total of six tasks (27 %). At the end of the training, there were no differences in motion or force parameters between the two groups. Group 2 rated their self-perceived dexterity after the training significantly lower than before the training and also reported significantly higher levels of frustration compared to group 1. Both groups rated the difficulty of the training similar.
Conclusion: Novices benefit from starting their training of difficult basic laparoscopic skills, e.g., suturing, in a transparent box trainer without camera. It takes less time to complete the tasks, and they get less frustrated by the training with the same results on their economy of movements and tissue handling skills.
Keywords: Endoscopy; Surgical; Technical; Training.
Figures

References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
