

HIV-associated large-vessel vasculopathy: a review of the current and emerging clinicopathological spectrum in vascular surgical practice
- PMID: 25940120
- PMCID: PMC4832607
- DOI: 10.5830/CVJA-2015-017
HIV-associated large-vessel vasculopathy: a review of the current and emerging clinicopathological spectrum in vascular surgical practice
Abstract
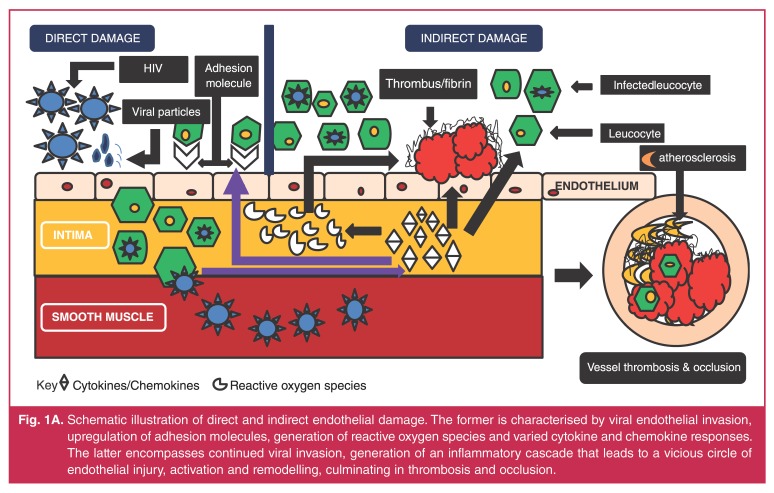
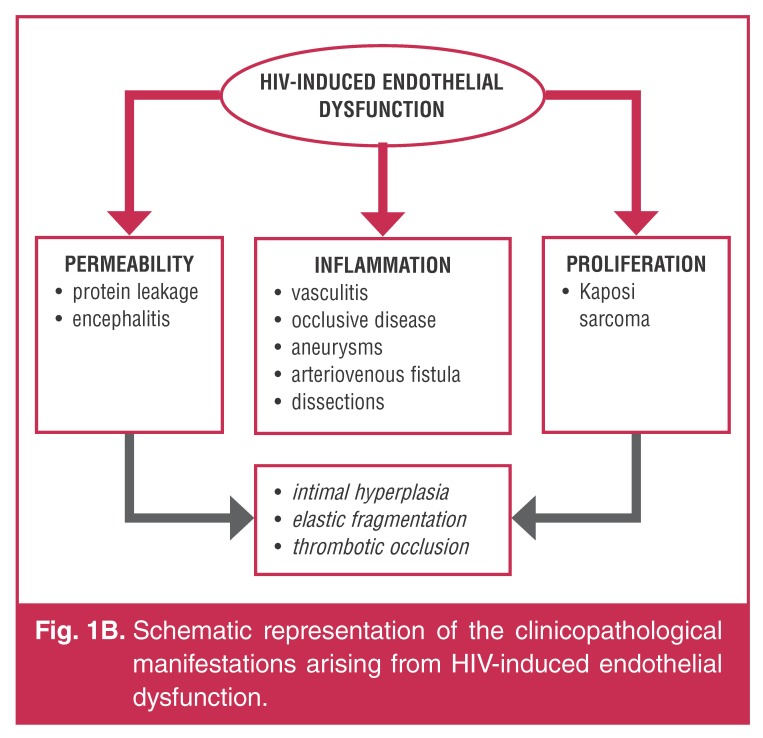
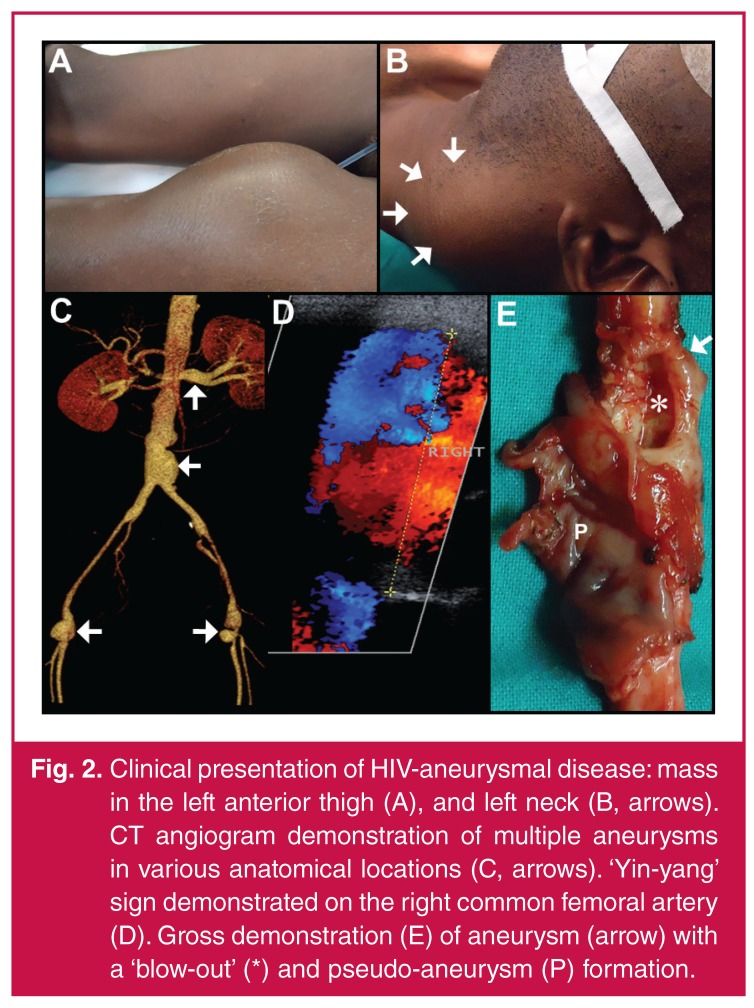
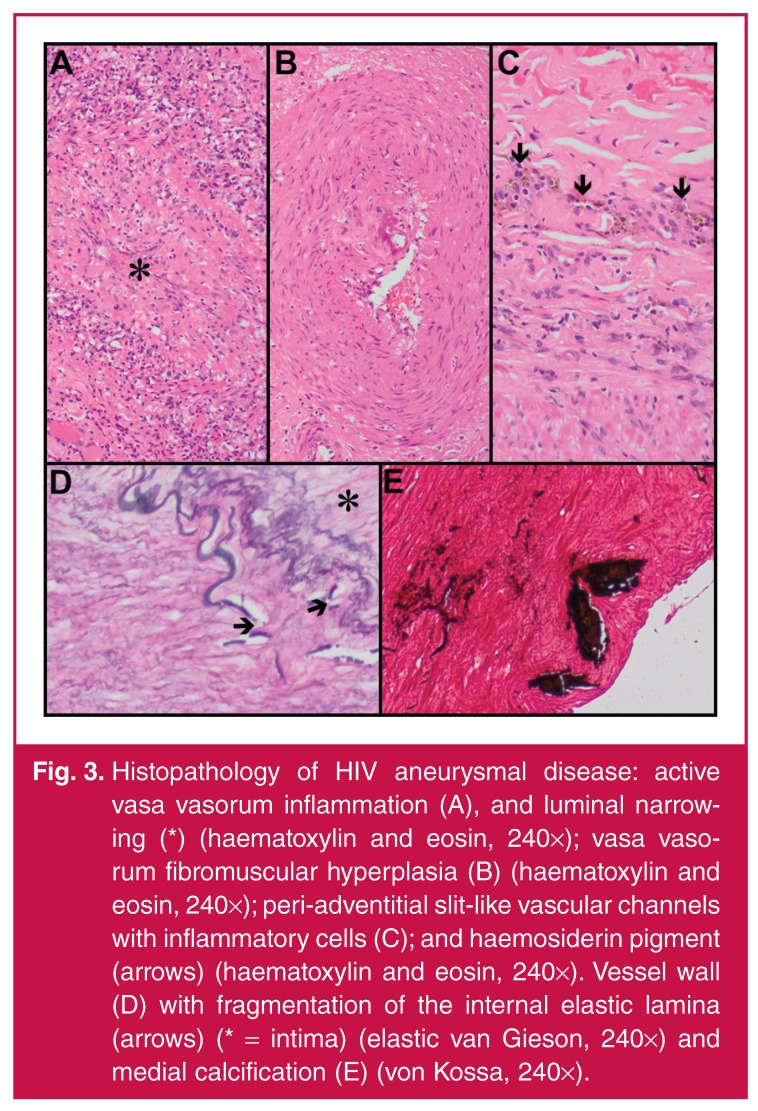
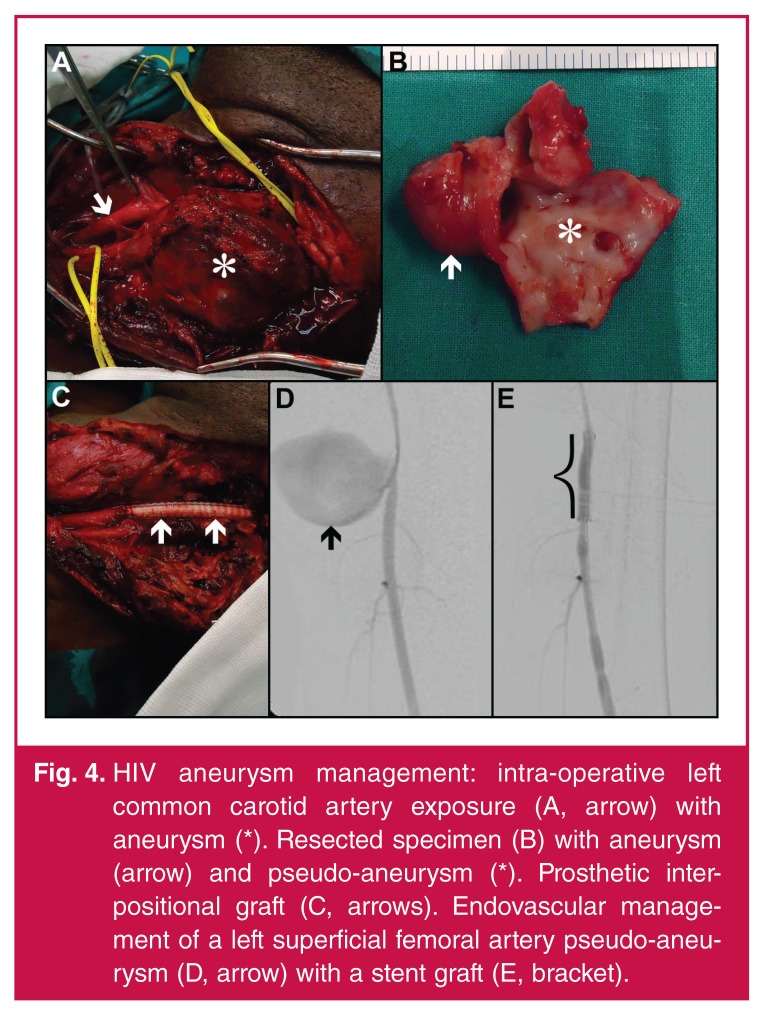
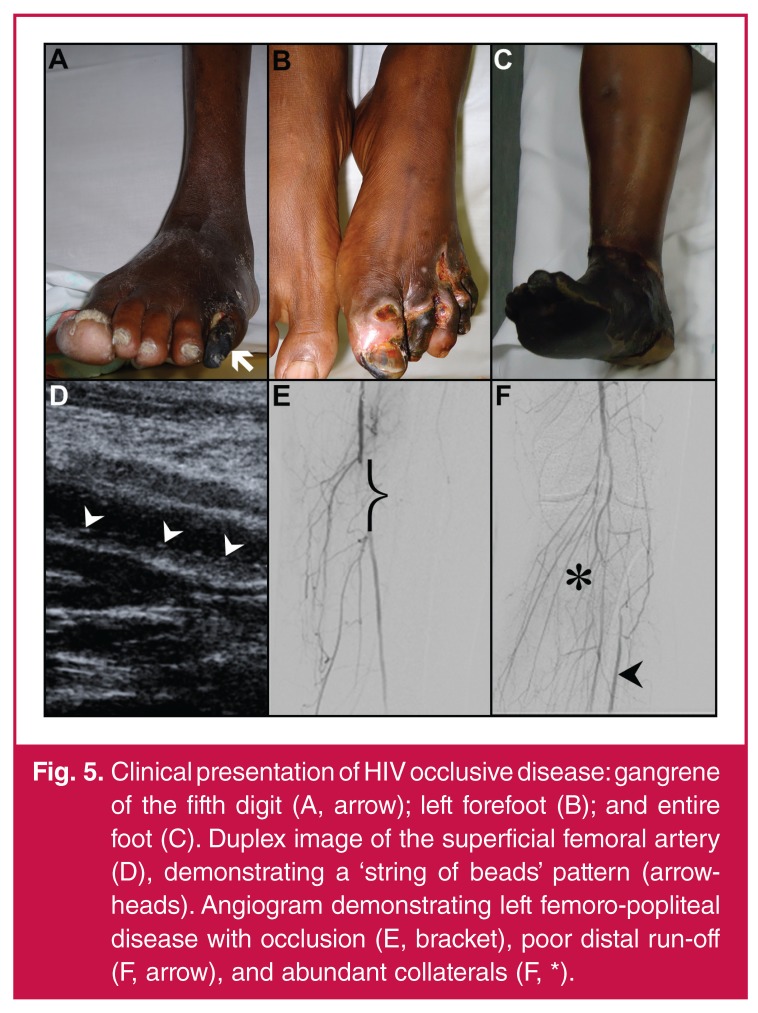
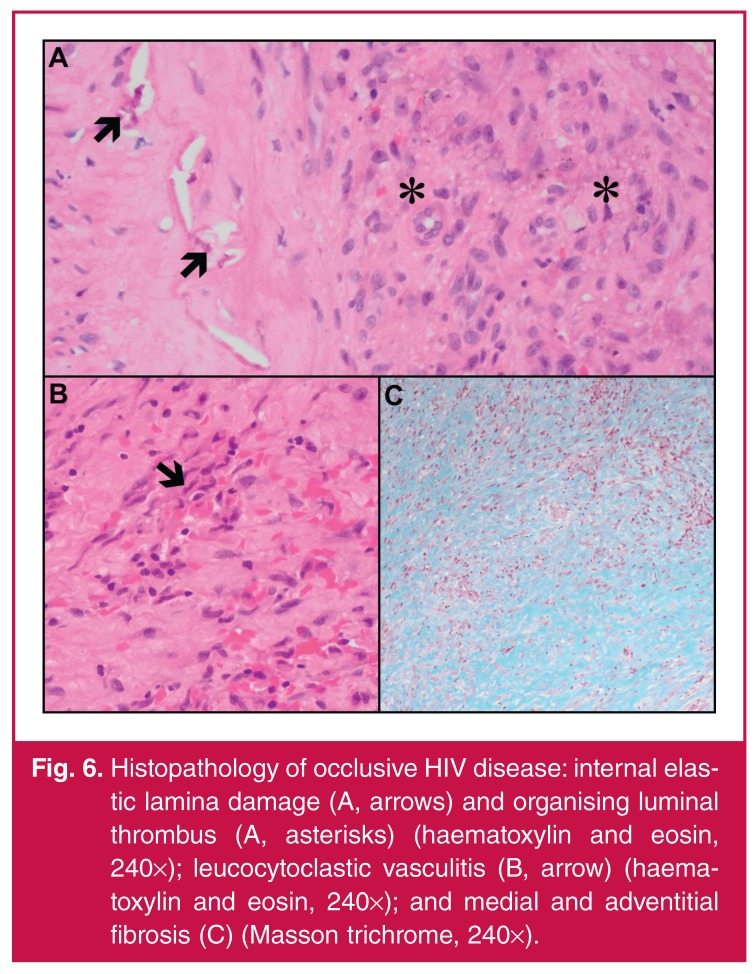
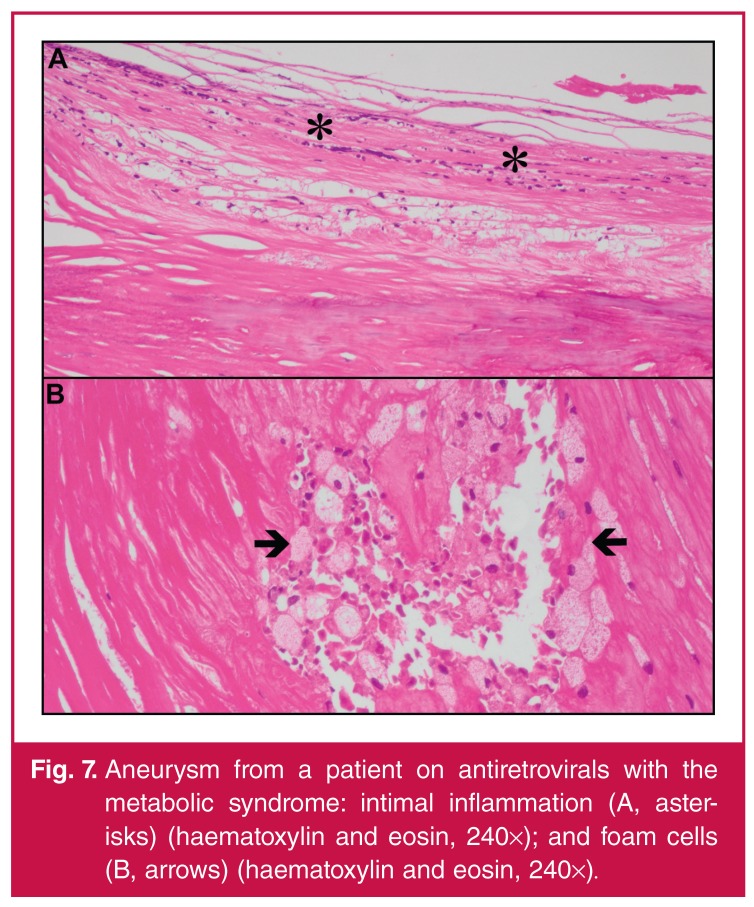
An established relationship exists between human immunodeficiency virus (HIV) and the vascular system, which is characterised by clinical expressions of aneurysmal and occlusive disease that emanate from a common pathological process. The exact pathogenesis is currently unknown; attempts to implicate opportunistic pathogens have been futile. Theories converge on leucocytoclastic vasculitis with the vaso vasora as the vasculopathic epicentre. It is thought that the virus itself or viral proteins trigger the release of inflammatory mediators that cause endothelial dysfunction and smooth muscle proliferation leading to vascular injury and thrombosis. The beneficial effects of highly active anti-retroviral therapy alter the natural history of the disease profile and promote longevity but are negated by cardiovascular complications. Atherosclerosis is an emerging challenge. Presently patients are managed by standard surgical protocols because of non-existent universal surgical interventional guidelines. Clinical response to treatment is variable and often compounded by complications of graft occlusion, sepsis and poor wound healing. The clinical, imaging and pathological observations position HIV-associated large-vessel vasculopathy as a unique entity. This review highlights the spectrum of HIV-associated large-vessel aneurysmal, occlusive and atherosclerotic disease in vascular surgical practice.
Figures
References
-
- Bennet NJ, Gilroy SA, Bronze MS, Glatt A, Windle ML. HIV disease. emedicine.medscape.com.2011.http://emedicine.medscape.com/article/211316... Accessed December 23/2013.
-
- Busari O, Opadijo O, Adeyemi O. Cardiac diseases in HIV and AIDS. Internet J Cardiol. 2008;5(2):1–13.
-
- Mulaudzi TV. HIV-associated vasculopathy. CME. 2009;27(7):320–322.
-
- Robbs JV, Paruk N. Management of HIV vasculopathy – a South African experience. Eur J Vasc Endovasc Surg. 2010;39(Suppl 1):S25–S31. - PubMed
-
- Joshi VV, Pawel B, Connor E. et al. Arteriopathy in children with acquired immune deficiency syndrome. Pediatr Pathol. 1987;7(3):261–275. - PubMed
Publication types
MeSH terms
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Medical