

Improved outcomes for emergency department patients whose ambulance off-stretcher time is not delayed
- PMID: 25940975
- PMCID: PMC4676924
- DOI: 10.1111/1742-6723.12399
Improved outcomes for emergency department patients whose ambulance off-stretcher time is not delayed
Abstract
Objective: To describe and compare characteristics and outcomes of patients who arrive by ambulance to the ED. We aimed to (i) compare patients with a delayed ambulance offload time (AOT) >30 min with those who were not delayed; and (ii) identify predictors of an ED length of stay (LOS) of >4 h for ambulance-arriving patients.
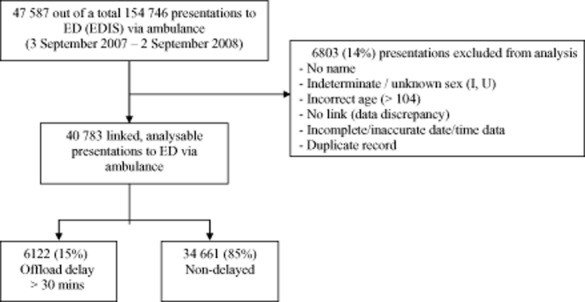
Methods: A retrospective, multi-site cohort study was undertaken in Australia using 12 months of linked health data (September 2007-2008). Outcomes of AOT delayed and non-delayed presentations were compared. Logistic regression analysis was undertaken to identify predictors of an ED LOS of >4 h.
Results: Of the 40 783 linked, analysable ambulance presentations, AOT delay of >30 min was experienced by 15%, and 63% had an ED LOS of >4 h. Patients with an AOT <30 min had better outcomes for: time to triage; ambulance time at hospital; time to see healthcare professional; proportion seen within recommended triage time frame; and ED LOS for both admitted and non-admitted patients. In-hospital mortality did not differ. Strong predictors of an ED LOS >4 h included: hospital admission, older age, triage category, and offload delay >30 min.
Conclusion: Patients arriving to the ED via ambulance and offloaded within 30 min experience better outcomes than those delayed. Given that offload delay is a modifiable predictor of an ED LOS of >4 h, targeted improvements in the ED arrival process for ambulance patients might be useful.
Keywords: ambulance; data linkage; emergency department; offload delay; outcome.
© 2015 The Authors. Emergency Medicine Australasia published by Wiley Publishing Asia Pty Ltd on behalf of Australasian College for Emergency Medicine and Australasian Society for Emergency Medicine.
Figures
References
-
- Hitchcock M, Crilly J, Gillespie B, Chaboyer W, Tippett V, Lind J. The effect of ambulance ramping on emergency department length of stay and in-patient mortality. Aust. Emerg. Nurs. J. 2010;13:17–24.
-
- Cooney DR, Millin MG, Carter A, Lawner BJ, Nable JV, Wallus HJ. Ambulance diversion and emergency department offload delay: resource document for the National Association of EMS Physicians Position Statement. Prehosp. Emer. Care. 2011;15:555–561. - PubMed
-
- Australian Institute of Health and Welfare (AIHW) Australian Hospital Statistics 2007–2008 Health Service Series no. 33. Cat. No. HSE 71. Canberra: AIHW; 2009.
-
- Institute of Medicine. Future of Emergency Care – Hospital-Based Emergency Care: At the Breaking Point. Washington, DC: National Academy Press; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
