

Portal vein thrombosis
- PMID: 25941431
- PMCID: PMC4415192
- DOI: 10.1016/j.jceh.2014.12.008
Portal vein thrombosis
Abstract
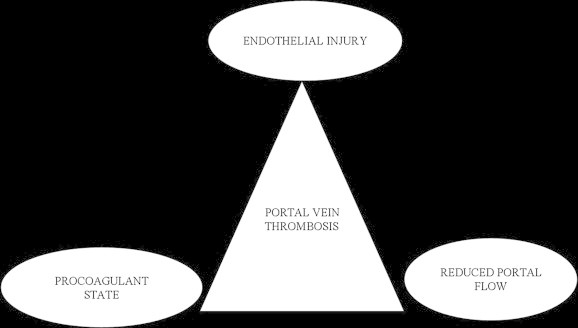
Portal vein thrombosis is an important cause of portal hypertension. PVT occurs in association with cirrhosis or as a result of malignant invasion by hepatocellular carcinoma or even in the absence of associated liver disease. With the current research into its genesis, majority now have an underlying prothrombotic state detectable. Endothelial activation and stagnant portal blood flow also contribute to formation of the thrombus. Acute non-cirrhotic PVT, chronic PVT (EHPVO), and portal vein thrombosis in cirrhosis are the three main variants of portal vein thrombosis with varying etiological factors and variability in presentation and management. Procoagulant state should be actively investigated. Anticoagulation is the mainstay of therapy for acute non-cirrhotic PVT, with supporting evidence for its use in cirrhotic population as well. Chronic PVT (EHPVO) on the other hand requires the management of portal hypertension as such and with role for anticoagulation in the setting of underlying prothrombotic state, however data is awaited in those with no underlying prothrombotic states. TIPS and liver transplant may be feasible even in the setting of PVT however proper selection of candidates and type of surgery is warranted. Thrombolysis and thrombectomy have some role. TARE is a new modality for management of HCC with portal vein invasion.
Keywords: ACLA, anti-cardiolipin antibody; AFP, alpha feto protein; BCS, Budd-Chiari syndrome; CDUS, color doppler ultrasonography; CT, computed tomography; CTP, Child Turcotte Pugh; EHPVO, extra hepatic portal venous obstruction; EST, endoscopic sclerotherapy; HCC, hepatocellular carcinoma; HVPG, hepatic venous pressure gradient; IGF-1, insulin like growth factor-1; IGFBP-3, insulin like growth factor binding protein-3; INR, international normalized ratio; JAK-2, Janus kinase 2; LA, lupus anticoagulant; LMWH, low molecular weight heparin; MELD, model for end stage liver disease; MPD, myeloproliferative disorder; MRI, magnetic resonance imaging; MTHFR, methylenetetrahydrofolate reductase; MVT, mesenteric vein thrombosis; OCPs, oral contraceptive pills; PAI-1 4G-4G, plasminogen activator inhibitor type 1- 4G/4G genotype; PNH, paroxysmal nocturnal hemoglobinuria; PV, portal vein; PVT; PVT, portal vein thrombosis; PWUS, Pulsed Wave ultrasonography; RFA, radio frequency ablation; SMA, superior mesenteric artery; SMV, superior mesenteric vein; TAFI, thrombin activatable fibrinolysis inhibitor; TARE, Trans arterial radioembolization; TB, tuberculosis; TIPS, transjugular intrahepatic portosystemic shunt; UFH, unfractionated heparin; acute and chronic; anticoagulation; imaging; prothrombotic; rtPA, recombinant tissue plasminogen activator.
Figures
References
-
- Okuda K., Ohnishi K., Kimura K. Incidence of portal vein thrombosis in liver cirrhosis. An angiographic study in 708 patients. Gastroenterology. 1985;89:279–286. - PubMed
-
- Gaiani S., Bolondi L., Li B.S., Zironi G., Siringo S., Barbara L. Prevalence of spontaneous hepatofugal portal flow in liver cirrhosis. Clinical and endoscopic correlation in 228 patients. Gastroenterology. 1991;100:160–167. - PubMed
-
- Manzanet G., Sanjuan F., Orbis P. Liver transplantation in patients with portal vein thrombosis. Liver Transpl. 2001;7:125–131. - PubMed
-
- Amitrano L., Guardascione M.A., Brancaccio V. Risk factors and clinical presentation of portal vein thrombosis in patients with liver cirrhosis. J Hepatol. 2004;40:736–741. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
Miscellaneous
