

Cost-Effectiveness of a Specialist Geriatric Medical Intervention for Frail Older People Discharged from Acute Medical Units: Economic Evaluation in a Two-Centre Randomised Controlled Trial (AMIGOS)
- PMID: 25942421
- PMCID: PMC4420253
- DOI: 10.1371/journal.pone.0121340
Cost-Effectiveness of a Specialist Geriatric Medical Intervention for Frail Older People Discharged from Acute Medical Units: Economic Evaluation in a Two-Centre Randomised Controlled Trial (AMIGOS)
Abstract
Background: Poor outcomes and high resource-use are observed for frail older people discharged from acute medical units. A specialist geriatric medical intervention, to facilitate Comprehensive Geriatric Assessment, was developed to reduce the incidence of adverse outcomes and associated high resource-use in this group in the post-discharge period.
Objective: To examine the costs and cost-effectiveness of a specialist geriatric medical intervention for frail older people in the 90 days following discharge from an acute medical unit, compared with standard care.
Methods: Economic evaluation was conducted alongside a two-centre randomised controlled trial (AMIGOS). 433 patients (aged 70 or over) at risk of future health problems, discharged from acute medical units within 72 hours of attending hospital, were recruited in two general hospitals in Nottingham and Leicester, UK. Participants were randomised to the intervention, comprising geriatrician assessment in acute units and further specialist management, or to control where patients received no additional intervention over and above standard care. Primary outcome was incremental cost per quality adjusted life year (QALY) gained.
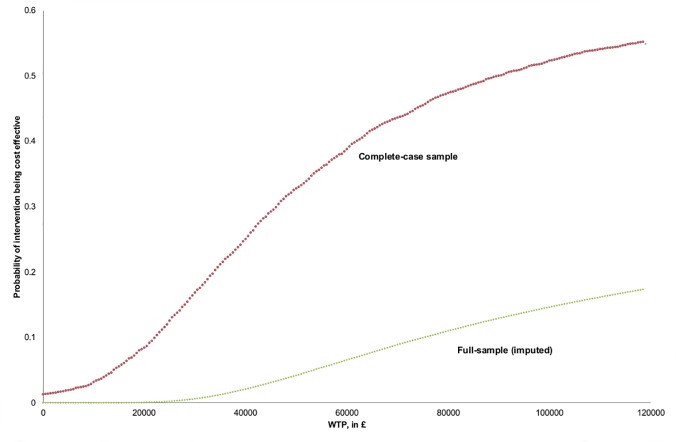
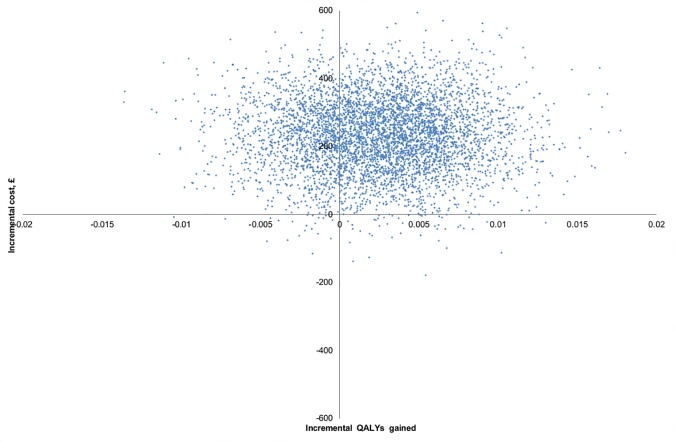
Results: We undertook cost-effectiveness analysis for 417 patients (intervention: 205). The difference in mean adjusted QALYs gained between groups at 3 months was -0.001 (95% confidence interval [CI]: -0.009, 0.007). Total adjusted secondary and social care costs, including direct costs of the intervention, at 3 months were £4412 (€5624, $6878) and £4110 (€5239, $6408) for the intervention and standard care groups, the incremental cost was £302 (95% CI: 193, 410) [€385, $471]. The intervention was dominated by standard care with probability of 62%, and with 0% probability of cost-effectiveness (at £20,000/QALY threshold).
Conclusions: The specialist geriatric medical intervention for frail older people discharged from acute medical unit was not cost-effective. Further research on designing effective and cost-effective specialist service for frail older people discharged from acute medical units is needed.
Trial registration: ISRCTN registry ISRCTN21800480 http://www.isrctn.com/ISRCTN21800480.
Conflict of interest statement
Figures
References
-
- Woodard J, Gladman J, Conroy S. Frail older people at the interface. Age Ageing. 2010;39(S1):i36.
-
- Ferguson C, Woodard J, Banerjee J, Conroy S. Operationalising frailty definitions in the emergency department-a mapping exercise. The Journal of Nutrition, Health and Ageing. 2009;13(Supplement 1):S266.
-
- Edmans J, Bradshaw L, Gladman JR, Franklin M, Berdunov V, Elliott R, et al. The Identification of Seniors at Risk (ISAR) score to predict clinical outcomes and health service costs in older people discharged from UK acute medical units. Age Ageing. 2013. Nov;42(6):747–53. Pubmed Central PMCID: PMC3809718. Epub 2013/05/15. eng. 10.1093/ageing/aft054 - DOI - PMC - PubMed
-
- Woodard J, Rowell G, Vartha R, Whittingham C, Vadher N, Conroy S. Appropriate prescribing in older people. J Nutr Health Aging. 2009;13(suppl 1):S477.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
