

Current concepts in targeting chronic obstructive pulmonary disease pharmacotherapy: making progress towards personalised management
- PMID: 25943943
- PMCID: PMC4869530
- DOI: 10.1016/S0140-6736(15)60693-6
Current concepts in targeting chronic obstructive pulmonary disease pharmacotherapy: making progress towards personalised management
Abstract
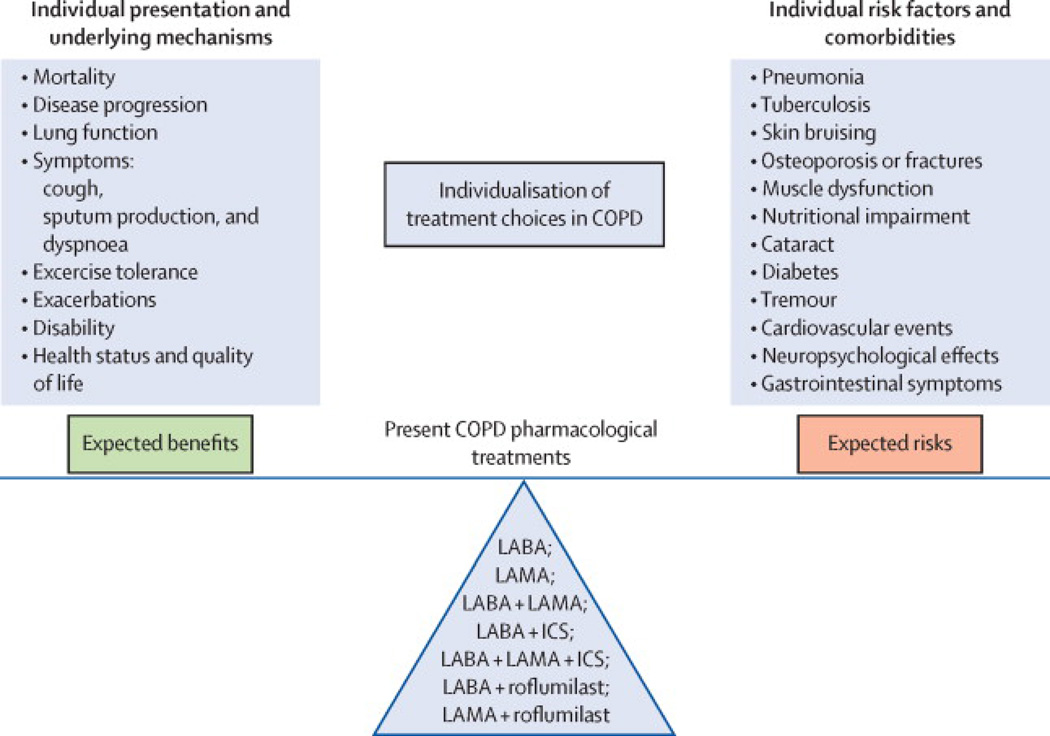
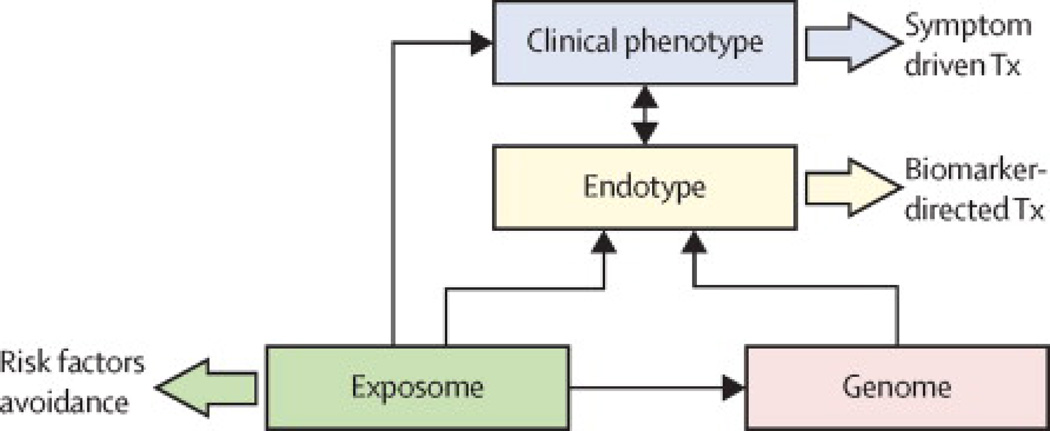
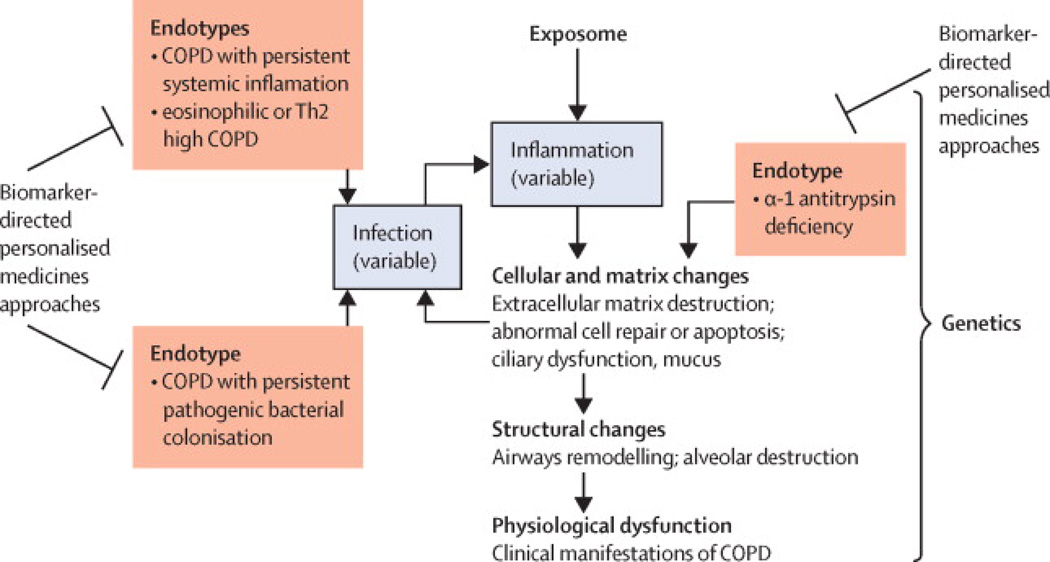
Chronic obstructive pulmonary disease (COPD) is a common, complex, and heterogeneous disorder that is responsible for substantial and growing morbidity, mortality, and health-care expense worldwide. Of imperative importance to decipher the complexity of COPD is to identify groups of patients with similar clinical characteristics, prognosis, or therapeutic needs, the so-called clinical phenotypes. This strategy is logical for research but might be of little clinical value because clinical phenotypes can overlap in the same patient and the same clinical phenotype could result from different biological mechanisms. With the goal to match assessment with treatment choices, the latest iteration of guidelines from the Global Initiative for Chronic Obstructive Lung Disease reorganised treatment objectives into two categories: to improve symptoms (ie, dyspnoea and health status) and to decrease future risk (as predicted by forced expiratory volume in 1 s level and exacerbations history). This change thus moves treatment closer to individualised medicine with available bronchodilators and anti-inflammatory drugs. Yet, future treatment options are likely to include targeting endotypes that represent subtypes of patients defined by a distinct pathophysiological mechanism. Specific biomarkers of these endotypes would be particularly useful in clinical practice, especially in patients in which clinical phenotype alone is insufficient to identify the underlying endotype. A few series of potential COPD endotypes and biomarkers have been suggested. Empirical knowledge will be gained from proof-of-concept trials in COPD with emerging drugs that target specific inflammatory pathways. In every instance, specific endotype and biomarker efforts will probably be needed for the success of these trials, because the pathways are likely to be operative in only a subset of patients. Network analysis of human diseases offers the possibility to improve understanding of disease pathobiological complexity and to help with the development of new treatment alternatives and, importantly, a reclassification of complex diseases. All these developments should pave the way towards personalised treatment of patients with COPD in the clinic.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Figures
References
-
- Vestbo J, Hurd SS, Agusti AG, Jones PW, Vogelmeier C, Anzueto A, Barnes PJ, Fabbri LM, Martinez FJ, Nishimura M, Stockley RA, Sin DD, Rodriguez-Roisin R. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. American Journal of Respiratory and Critical Care Medicine. 2013;187:347–365. - PubMed
-
- Agusti A. The path to personalised medicine in COPD. Thorax. 2014;69:857–864. - PubMed
-
- Han MK, Agusti A, Calverley PM, Celli BR, Criner G, Curtis JL, Fabbri LM, Goldin JG, Jones PW, Macnee W, Make BJ, Rabe KF, Rennard SI, Sciurba FC, Silverman EK, Vestbo J, Washko GR, Wouters EF, Martinez FJ. Chronic obstructive pulmonary disease phenotypes: the future of COPD. American Journal of Respiratory and Critical Care Medicine. 2010;182:598–604. - PMC - PubMed
-
- Lotvall J, Akdis CA, Bacharier LB, Bjermer L, Casale TB, Custovic A, Lemanske RF, Jr, Wardlaw AJ, Wenzel SE, Greenberger PA. Asthma endotypes: a new approach to classification of disease entities within the asthma syndrome. The Journal of Allergy and Clinical Immunology. 2011;127:355–360. - PubMed
-
- Agusti A, Calverley PM, Celli B, Coxson HO, Edwards LD, Lomas DA, MacNee W, Miller BE, Rennard S, Silverman EK, Tal-Singer R, Wouters E, Yates JC, Vestbo J Evaluation of, COPD Longitudinally to Identify Predictive Surrogate Endpoints investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respiratory Research. 2010;11:122. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
