

Volume overload and adverse outcomes in chronic kidney disease: clinical observational and animal studies
- PMID: 25944876
- PMCID: PMC4599419
- DOI: 10.1161/JAHA.115.001918
Volume overload and adverse outcomes in chronic kidney disease: clinical observational and animal studies
Abstract
Background: Volume overload is frequently encountered and is associated with cardiovascular risk factors in patients with chronic kidney disease (CKD). However, the relationship between volume overload and adverse outcomes in CKD is not fully understood.
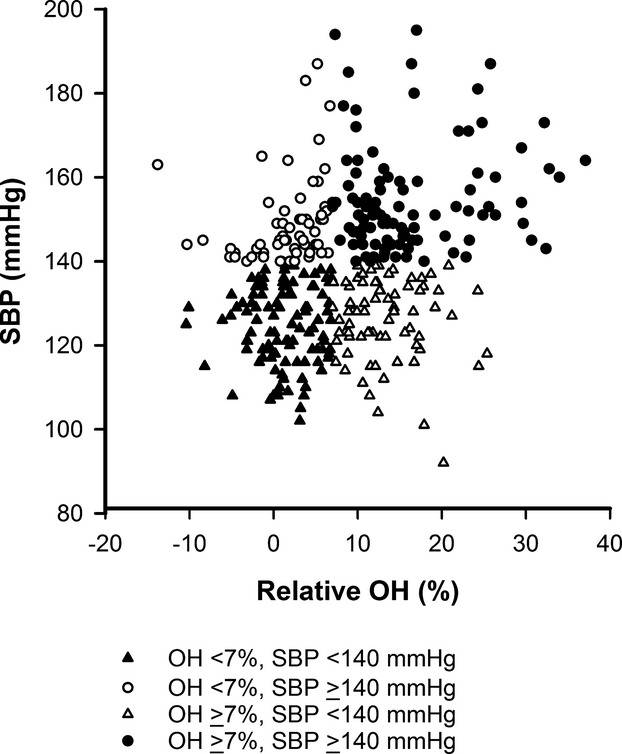
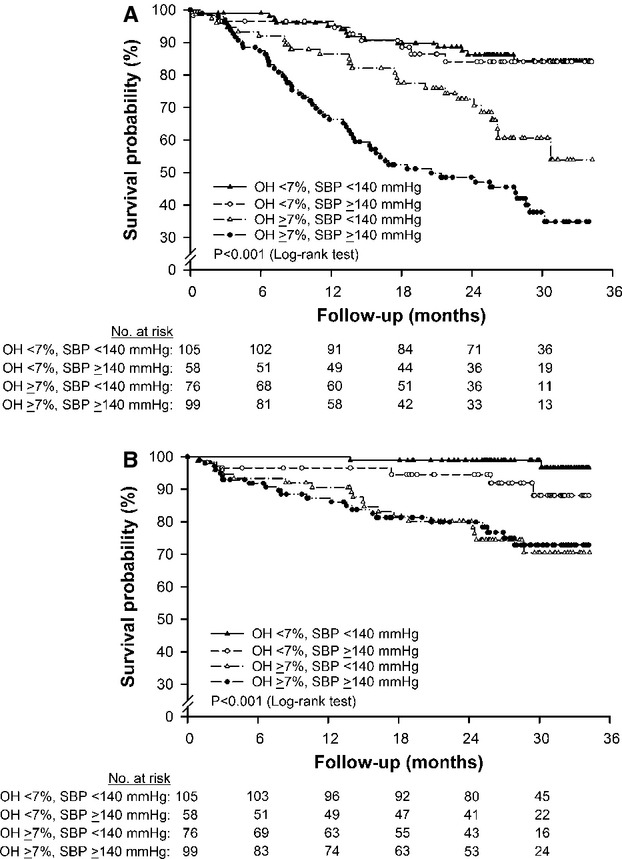
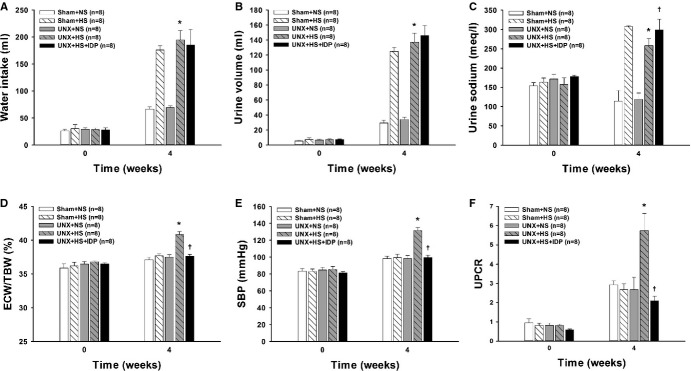
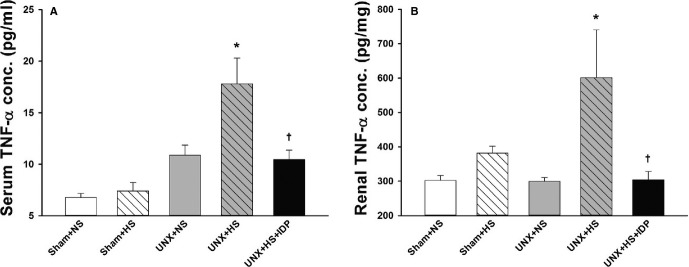
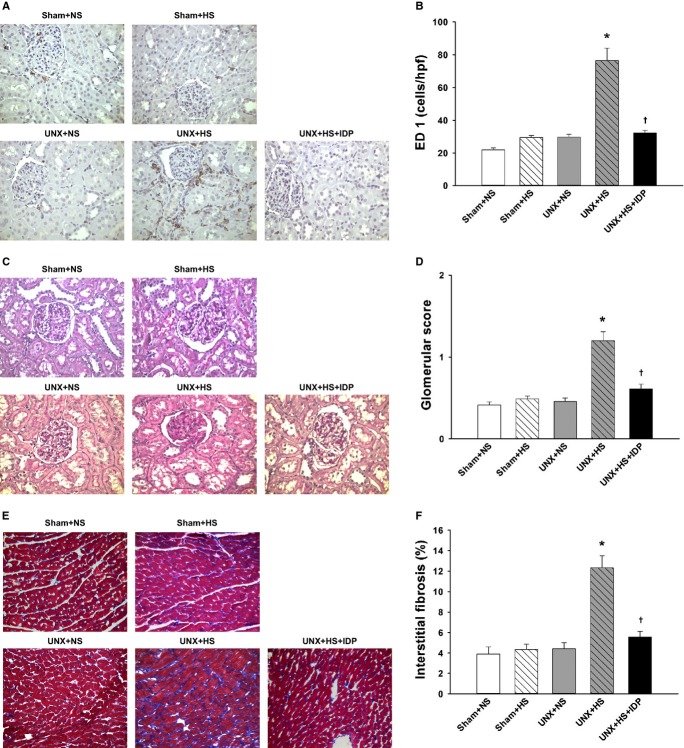
Methods and results: A prospective cohort of 338 patients with stage 3 to 5 CKD was followed for a median of 2.1 years. The study participants were stratified by the presence or absence of volume overload, defined as an overhydration index assessed by bioimpedance spectroscopy exceeding 7%, the 90th percentile for the healthy population. The primary outcome was the composite of estimated glomerular filtration rate decline ≥50% or end-stage renal disease. The secondary outcome included a composite of morbidity and mortality from cardiovascular causes. Animal models were used to simulate fluid retention observed in human CKD. We found that patients with volume overload were at a higher risk of the primary and secondary end points in the adjusted Cox models. Furthermore, overhydration appears to be more important than hypertension in predicting an elevated risk. In rats subjected to unilateral nephrectomy and a high-salt diet, the extracellular water significantly increased. This fluid retention was associated with an increase in blood pressure, proteinuria, renal inflammation with macrophage infiltration and tumor necrosis factor-α overexpression, glomerular sclerosis, and cardiac fibrosis. Diuretic treatment with indapamide attenuated these changes, suggesting that fluid retention might play a role in the development of adverse outcomes.
Conclusions: Volume overload contributes to CKD progression and cardiovascular diseases. Further research is warranted to clarify whether the correction of volume overload would improve outcomes for CKD patients.
Keywords: bioimpedance; cardiovascular disease; chronic kidney disease; hypertension; overhydration; volume overload.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Levey AS, Atkins R, Coresh J, Cohen EP, Collins AJ, Eckardt KU, Nahas ME, Jaber BL, Jadoul M, Levin A, Powe NR, Rossert J, Wheeler DC, Lameire N, Eknoyan G. Chronic kidney disease as a global public health problem: approaches and initiatives—a position statement from Kidney Disease Improving Global Outcomes. Kidney Int. 2007;72:247–259. - PubMed
-
- Wen CP, Cheng TY, Tsai MK, Chang YC, Chan HT, Tsai SP, Chiang PH, Hsu CC, Sung PK, Hsu YH, Wen SF. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462293 adults in Taiwan. Lancet. 2008;371:2173–2182. - PubMed
-
- Hsu TW, Liu JS, Hung SC, Kuo KL, Chang YK, Chen YC, Hsu CC, Tarng DC. Renoprotective effect of renin-angiotensin system blockade among advanced chronic kidney disease non-dialyzed patients with hypertension and anemia. JAMA Intern Med. 2014;174:347–354. - PubMed
-
- Chen YR, Yang Y, Wang SC, Chiu PF, Chou WY, Lin CY, Chang JM, Chen TW, Ferng SH, Lin CL. Effectiveness of multidisciplinary care for chronic kidney disease in Taiwan: a 3-year prospective cohort study. Nephrol Dial Transplant. 2013;28:671–682. - PubMed
-
- Hung SC, Kuo KL, Peng CH, Wu CH, Wang YC, Tarng DC. Association of fluid retention with anemia and clinical outcomes among patients with chronic kidney disease. J Am Heart Assoc. 2015;4:e001480. doi: 10.1161/JAHA.114.001480. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
