

Peripheral Dendritic Cells and CD4+CD25+Foxp3+ Regulatory T Cells in the First Trimester of Normal Pregnancy and in Women with Recurrent Miscarriage
- PMID: 25945787
- PMCID: PMC4422710
- DOI: 10.1371/journal.pone.0124747
Peripheral Dendritic Cells and CD4+CD25+Foxp3+ Regulatory T Cells in the First Trimester of Normal Pregnancy and in Women with Recurrent Miscarriage
Abstract
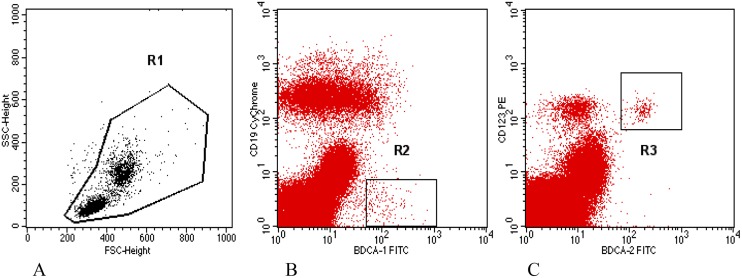
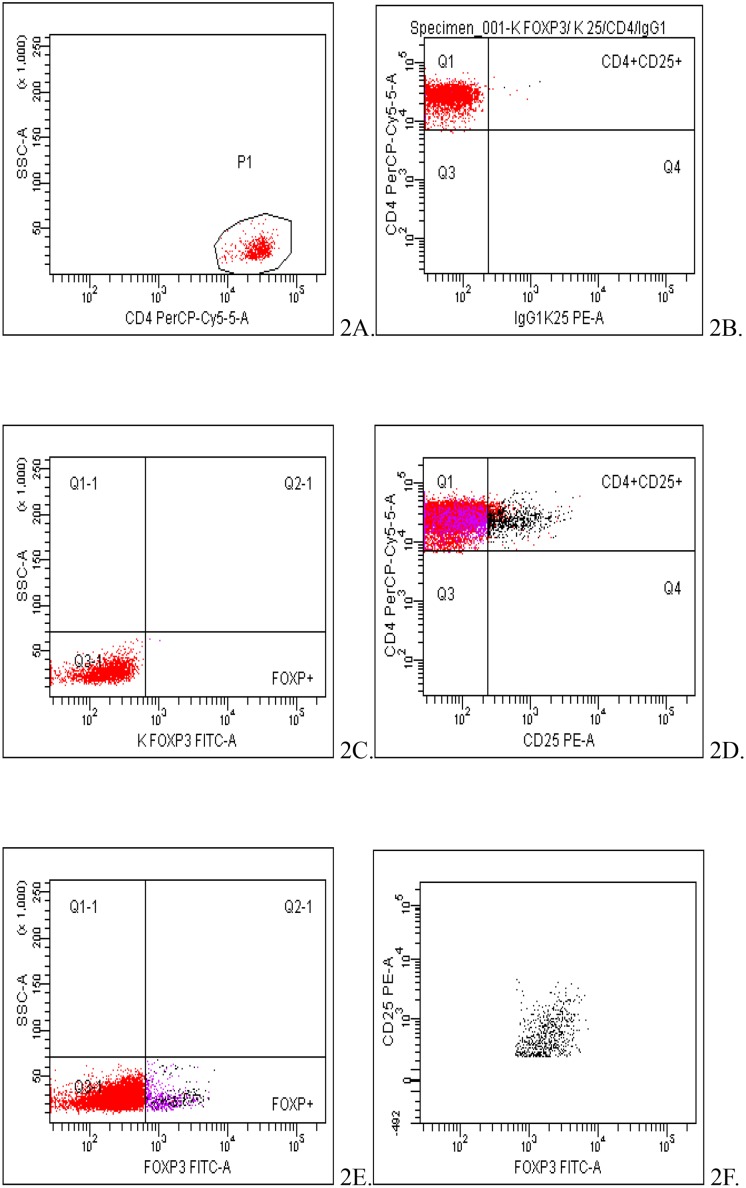
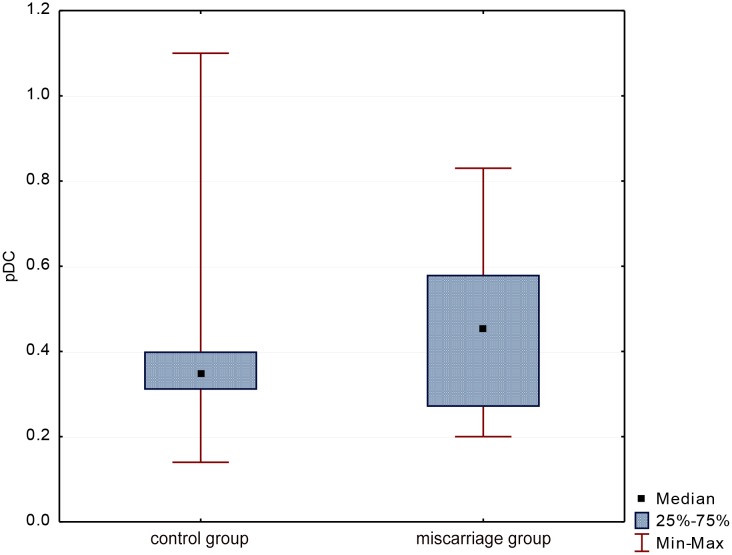
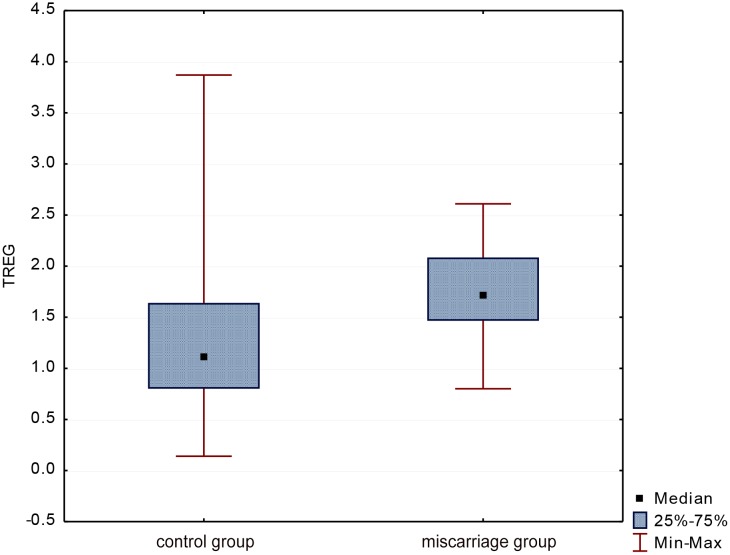
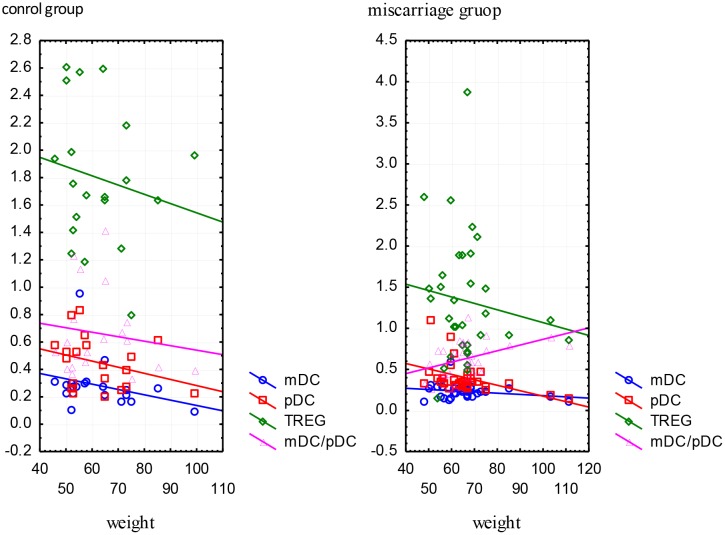
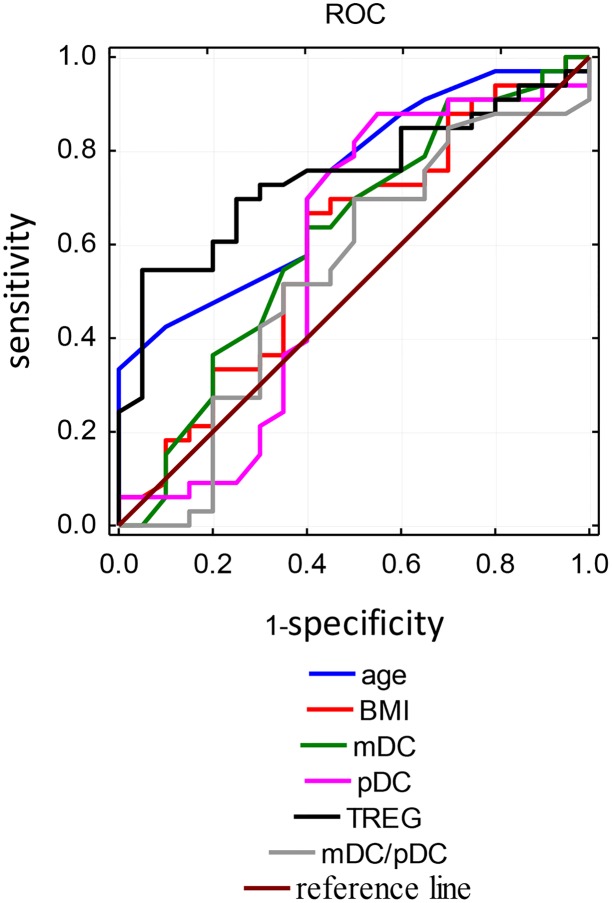
The development of pregnancy is possible due to initiation of immune response in the body of the mother resulting in immune tolerance. Miscarriage may be caused by the impaired maternal immune response to paternal alloantigens located on the surface of trophoblast and fetal cells. The aim of the study was to compare the population of circulating dendritic cells (DCs) and CD4+CD25+Foxp3+ regulatory T cells (TREGs) in the first trimester of a normal pregnancy and in women with recurrent miscarriage and an attempt to determine the relationship between these cells and the role they may play in human reproductive failures. The study was conducted in a group of 33 first trimester pregnant women with recurrent miscarriage and in a group of 20 healthy pregnant women in the first trimester of normal pregnancy. Among mononuclear cells isolated from peripheral blood, the populations of DCs and TREGs were assessed by flow cytometry. The percentage of myeloid DCs and lymphoid DCs showed no significant difference between study and control group. Older maternal age and obesity significantly reduced the pool of circulating myeloid and lymphoid DCs (R=-0.39, p=0.02). In miscarriages the percentage of circulating TREGs was significantly lower compared to normal pregnancies (p=0.003). Among the analysed factors the percentage of TREGs was the most sensitive and the most specific parameter which correlated with the pregnancy loss. The reduction in the population of circulating TREGs suggests immunoregulatory mechanisms disorder in a pregnancy complicated by miscarriage.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
