

Preterm or not--an evaluation of estimates of gestational age in a cohort of women from Rural Papua New Guinea
- PMID: 25945927
- PMCID: PMC4422681
- DOI: 10.1371/journal.pone.0124286
Preterm or not--an evaluation of estimates of gestational age in a cohort of women from Rural Papua New Guinea
Abstract
Background: Knowledge of accurate gestational age is required for comprehensive pregnancy care and is an essential component of research evaluating causes of preterm birth. In industrialised countries gestational age is determined with the help of fetal biometry in early pregnancy. Lack of ultrasound and late presentation to antenatal clinic limits this practice in low-resource settings. Instead, clinical estimators of gestational age are used, but their accuracy remains a matter of debate.
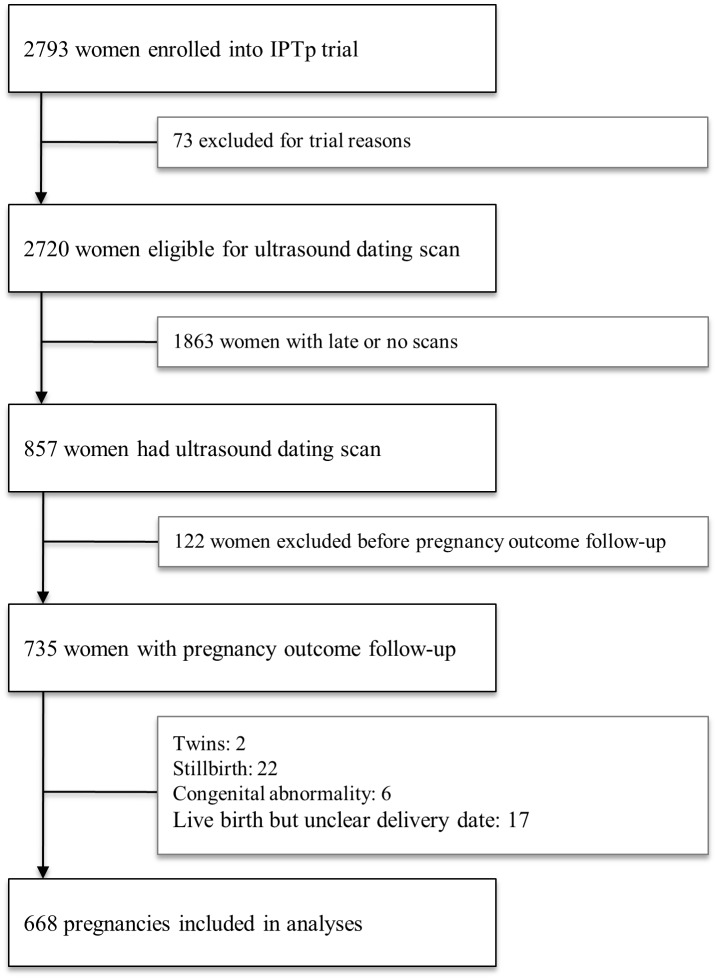
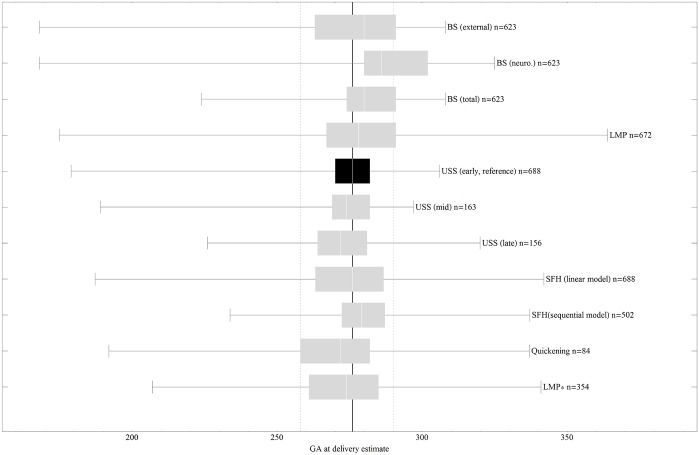
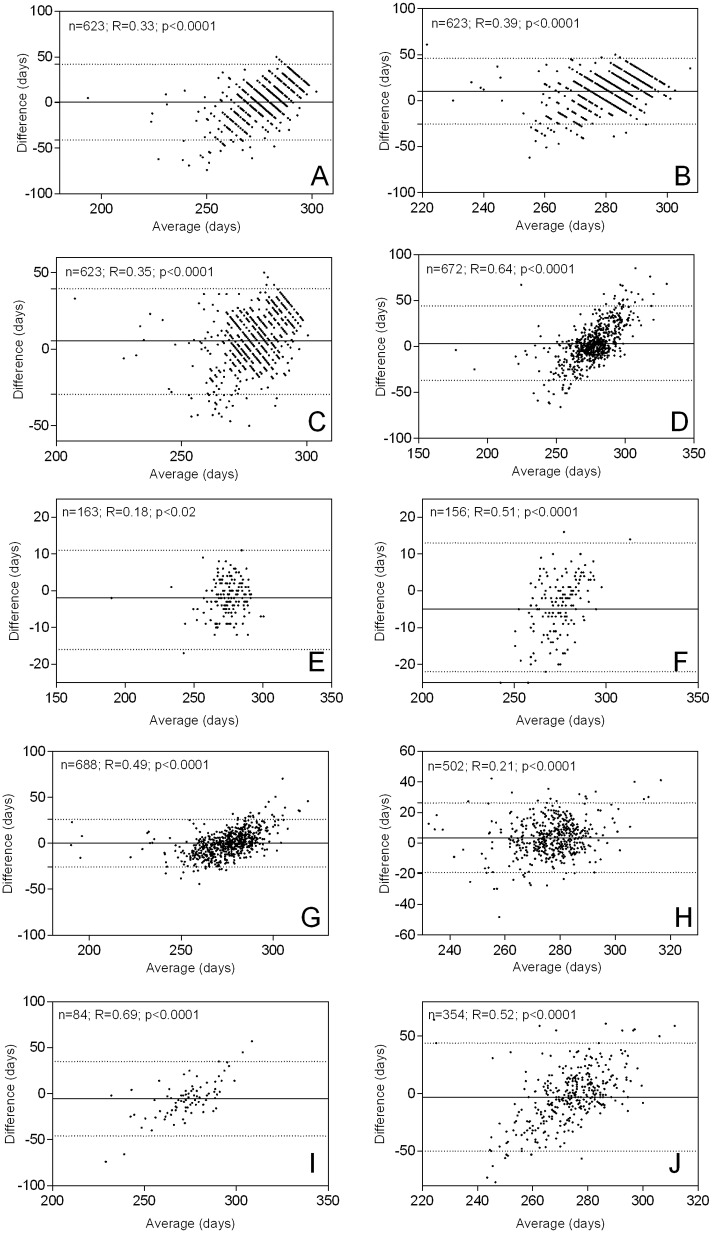
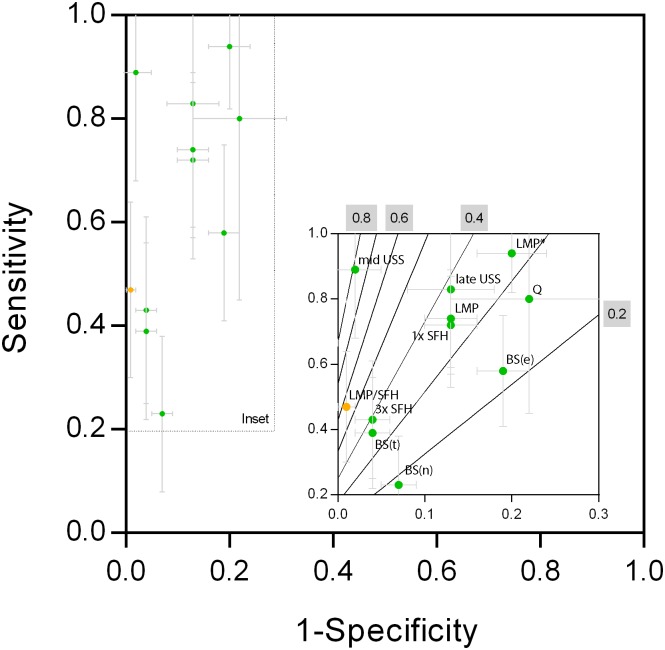
Methods: In a cohort of 688 singleton pregnancies from rural Papua New Guinea, delivery gestational age was calculated from Ballard score, last menstrual period, symphysis-pubis fundal height at first visit and quickening as well as mid- and late pregnancy fetal biometry. Published models using sequential fundal height measurements and corrected last menstrual period to estimate gestational age were also tested. Novel linear models that combined clinical measurements for gestational age estimation were developed. Predictions were compared with the reference early pregnancy ultrasound (<25 gestational weeks) using correlation, regression and Bland-Altman analyses and ranked for their capability to predict preterm birth using the harmonic mean of recall and precision (F-measure).
Results: Average bias between reference ultrasound and clinical methods ranged from 0-11 days (95% confidence levels: 14-42 days). Preterm birth was best predicted by mid-pregnancy ultrasound (F-measure: 0.72), and neuromuscular Ballard score provided the least reliable preterm birth prediction (F-measure: 0.17). The best clinical methods to predict gestational age and preterm birth were last menstrual period and fundal height (F-measures 0.35). A linear model combining both measures improved prediction of preterm birth (F-measure: 0.58).
Conclusions: Estimation of gestational age without ultrasound is prone to significant error. In the absence of ultrasound facilities, last menstrual period and fundal height are among the more reliable clinical measures. This study underlines the importance of strengthening ultrasound facilities and developing novel ways to estimate gestational age.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
